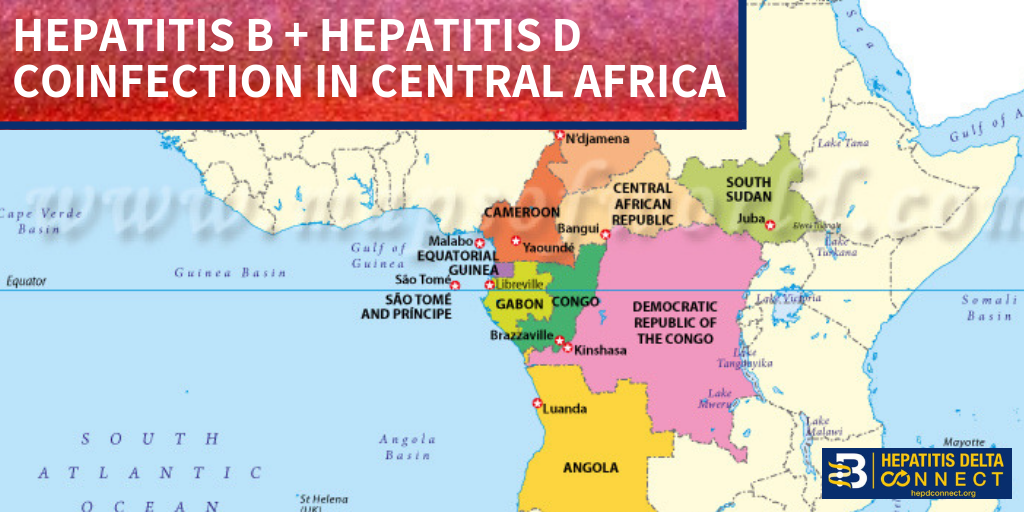
This Liver Cancer Awareness Month, we are connecting the dots between hepatitis B and liver cancer. Hepatitis B is responsible for up to 60% of all liver cancer cases worldwide. In fact, some of the highest rates of liver cancer are found in places with extremely high rates of hepatitis B, such as sub-Saharan Africa and Southeast Asia. Although liver cancer is the sixth most common cancer in the world, it is the second most common cause of cancer deaths. Liver cancer prevention should be a priority for all living with hepatitis B. Luckily, there are steps that you can take to prevent liver cancer – whether you are living with hepatitis B or not!
The Importance of Regular Check-Ups
Did you know that a chronic hepatitis B infection can lead to liver cancer without signs of previous damage such as cirrhosis? Many people do not realize that chronic hepatitis B is the primary global risk factor for developing liver cancer. Cirrhosis – or scarring or the liver – is often a risk factor for liver cancer, but it is not always the case for those living with hepatitis B. This is one of the reasons why it is so important for family members and sexual partners of infected individuals to get tested as well! Lack of symptoms does not mean that damage is not occurring.
Visiting a doctor regularly is the best way to prevent liver cancer if you are living with hepatitis B. The standard recommendation for visiting your doctor is every six months however this can vary based upon the severity of your infection. The doctor will take a few blood tests, along with an ultrasound examination of the abdominal area to determine the health of the liver. Based upon these tests and other risk factors, the doctor will be able to determine if liver damage is occurring and can guide you on which steps you should take next.
If damage is detected early enough, progression to liver cancer can be prevented through highly effective treatments that stop or slow the virus from reproducing in your liver. However, it is important to note that not everyone living with hepatitis B needs treatment. Current treatments have been proven to be most effective when there are signs of active liver damage. Hepatitis B can be managed through regular monitoring by a knowledgeable doctor and lifestyle changes that can go a long way in protecting your body.
Early detection of liver cancer is extremely important. The average 5-year survival rate once diagnosed with liver cancer ranges from 10% -14%. However, with early detection and proper treatment, those numbers rise to over 50%! This significant difference is because if liver cancer is caught early, a doctor can link you to life-saving treatments including chemotherapy, surgical options, ablation techniques, intra-arterial therapies or a liver transplant. Regular monitoring by a knowledgeable doctor will hopefully identify the markers of liver cancer before it occurs, but if you are living with liver cancer, there are treatment options and resources available to you.
Preventing Liver Cancer
Educating oneself is the first step in prevention! If you have hepatitis B, be aware of the risk factors and behaviors that can increase your likelihood of liver damage and liver cancer, such as consuming alcohol and high amounts of junk food, and lack of exercise. Non-Alcoholic Fatty Liver Disease (NAFLD) can also increase your risk of cancer, so it is important to discuss NAFLD risk factors and prevention tips with your doctor. Groups such as the CDC Division of Viral Hepatitis and the American Association for the Study of Liver Diseases all provide free fact sheets, call lines, and literature by experts that can help you understand what may be occurring in your body and to make educated choices. You can also check out our Liver Cancer Connect resource for more information or for liver cancer support.
The hepatitis B vaccine is also the first anti-cancer vaccine ever created! Remember that the vaccine is typically given in a set of 3 doses. It is extremely important to take all three in order to receive lifelong protection from hepatitis B-related liver cancer. In the U.S., there is also a 2-dose vaccine available, so you can be fully protected with fewer doses! If you are worried about the cost of the birth dose for your infant or the vaccine for yourself, many countries have free health clinics that can administer it or link you to an organization that can help.
Another key to preventing liver cancer is to get tested for hepatitis B. If you have not received your vaccine and you think you fall into a high-risk group, talk to your doctor about getting tested. Because hepatitis B often has no symptoms, it is important to get screened even if you do not feel ill. An early diagnosis means that you can begin any needed treatment sooner and prevent irreversible damage from occurring. Like the vaccines, your local doctor or health clinic may be able to test you for free or reduced cost – just ask! Some local community groups also provide free hepatitis B testing, so be sure to look out for flyers and announcements about them in your community as well



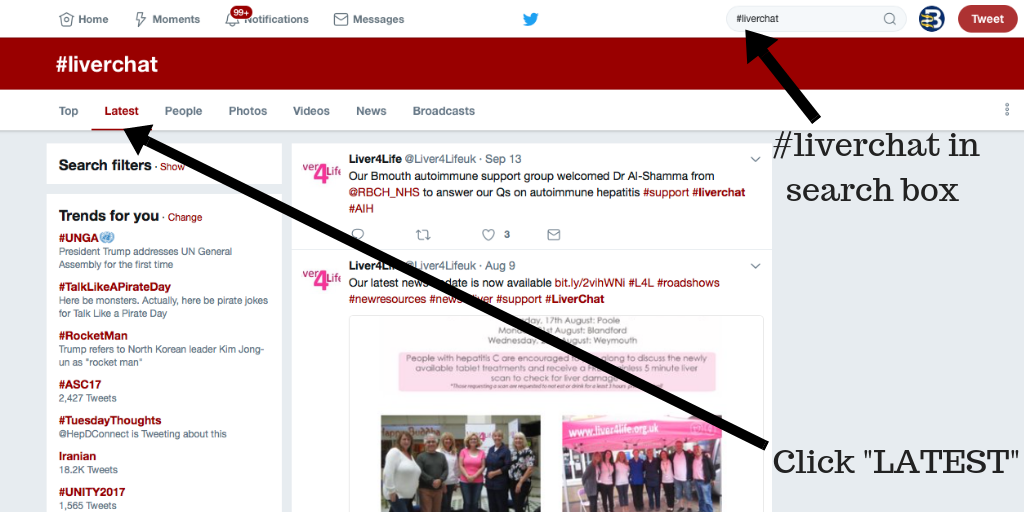
 October is Liver Cancer Awareness Month. Often we neglect to think about the link between hepatitis and liver cancer. Tuesday, Oct. 16, representatives from
October is Liver Cancer Awareness Month. Often we neglect to think about the link between hepatitis and liver cancer. Tuesday, Oct. 16, representatives from