
By Sierra Pellechio, Hepatitis Delta Connect Coordinator
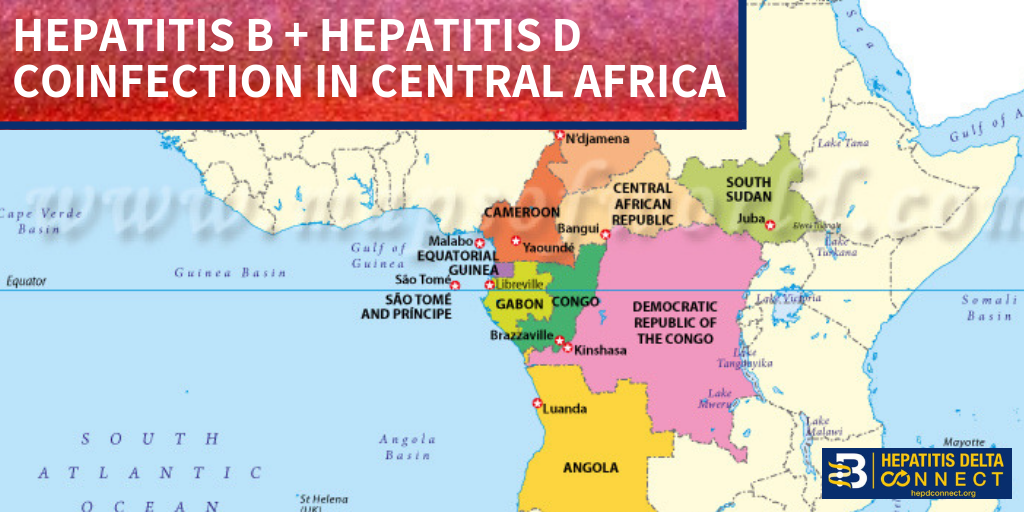
Since the 1990’s most of Eastern Europe has seen a decline in the prevalence of hepatitis D, a dangerous coinfection of hepatitis B, attributed to successful vaccination programs and government prioritization. Romania, which has the highest hepatitis B prevalence in the EU, has not seen such declines of hepatitis D, which affects 23% of its hepatitis B patients. Hepatitis D coinfection is considered hyperendemic to the country, and has some of the highest rates of coinfection globally1. Seventy percent of these 200,000 patients will progress to cirrhosis, often within only 10 years2, and face barriers to receiving effective treatment and management. Although the country enacted a national hepatitis B vaccination program for all newborns in 1995 and a catch-up program for school-age children in 1999, older populations already infected with hepatitis B and inadequately immunized young people represent susceptible groups for coinfection with hepatitis B and disease.1,3. Additionally; lack of hepatitis B vaccination recommendations for high risk groups, low implementation of hepatitis B screening during pregnancy, supply shortages and vaccine hesitancy, have created opportunities for hepatitis B and D transmission. Exposure to infected blood or sexual fluids through blood transfusions or surgeries (before the 1990’s), tattoos, piercings, injection drug use, or sexual contact with an infected person, can expose people already living with hepatitis B to hepatitis D, or expose those who have not received the full hepatitis B vaccine series to both viruses. Control of hepatitis B and D coinfection has also been hindered by the lack of a national registry and surveillance system thus preventing an understanding of the accurate prevalence and public health burden1.
disease.1,3. Additionally; lack of hepatitis B vaccination recommendations for high risk groups, low implementation of hepatitis B screening during pregnancy, supply shortages and vaccine hesitancy, have created opportunities for hepatitis B and D transmission. Exposure to infected blood or sexual fluids through blood transfusions or surgeries (before the 1990’s), tattoos, piercings, injection drug use, or sexual contact with an infected person, can expose people already living with hepatitis B to hepatitis D, or expose those who have not received the full hepatitis B vaccine series to both viruses. Control of hepatitis B and D coinfection has also been hindered by the lack of a national registry and surveillance system thus preventing an understanding of the accurate prevalence and public health burden1.
With health expenditure and life expectancy the lowest in the EU, Romania is battling large system-wide failures that have fostered the persistence of hepatitis B and D in its population5.
Dr. Florin Caruntu, of the National Institute of Infectious Diseases in Bucharest, has suggested that there is a general low level of awareness and screening among health care providers in Romania,  which has led to late diagnoses and cost many patient lives. For patients who are diagnosed, investigational testing is not covered by the national insurance house, placing a financial burden on patients to pay out of pocket for the additional testing necessary to manage their coinfection. With pegylated interferon injections as the only semi-effective treatment option, even diagnosed patients struggle to effectively control their coinfection and even less are connected to clinical trials. Although there are 7 new drugs in clinical trials, progress has lagged behind patient need for new therapies, many of whom are living with cirrhosis.
which has led to late diagnoses and cost many patient lives. For patients who are diagnosed, investigational testing is not covered by the national insurance house, placing a financial burden on patients to pay out of pocket for the additional testing necessary to manage their coinfection. With pegylated interferon injections as the only semi-effective treatment option, even diagnosed patients struggle to effectively control their coinfection and even less are connected to clinical trials. Although there are 7 new drugs in clinical trials, progress has lagged behind patient need for new therapies, many of whom are living with cirrhosis.
Increased government investment in the healthcare system, including medical training and education programs for provider awareness, updated protocols and coverage of investigational testing, would pave the way for increased patient identification and navigation to successful care. As clinical trials continue to progress, it is critical that Romania be a top consideration for clinical trial sites, as patients anxiously await more effective treatment options.
For more information on HDV in Romania, please watch our webinar featuring expert speaker, Dr. Florin Caruntu, of the National Institute of Infectious Diseases in Bucharest, Romania.
For more information about hepatitis B/D coinfection and the Hepatitis Delta Connect program, please visit www.hepdconnect.org or email us at connect@hepdconnect.org. If you are a hepatitis delta patient, and wish to receive information about upcoming clinical trials, please enter your information here. Hepatitis Delta Connect seeks to provide information, resources and support for hepatitis B/D patients and their families through its website, social media, fact sheets, webinars and hepatitis D liver specialist directory.
1. Hepatitis delta virus infection in Romania: Prevalence and risk factors. (2015). Journal of Gastrointestinal and Liver Diseases, 24(4) doi:10.15403/jgld.2014.1121.244.dtv
2. Noureddin, M., & Gish, R. (2014). Hepatitis delta: Epidemiology, diagnosis and management 36 Years after discovery. Current Gastroenterology Reports, 16(1), 1-8. doi:10.1007/s11894-013-0365-x
3. Ruta, S. M., Matusa, R. F., Sultana, C., Manolescu, L., Kozinetz, C. A., Kline, M. W., & Cernescu, C. (2005). High prevalence of hepatitis B virus markers in Romanian adolescents with human immunodeficiency virus infection. Journal of the International AIDS Society, 7(1), 68-68. doi:10.1186/1758-2652-7-1-68
4. Gheorghe, L., Csiki, I. E., Iacob, S., & Gheorghe, C. (2013). The prevalence and risk factors of hepatitis B virus infection in an adult population in Romania: A nationwide survey. European Journal of Gastroenterology & Hepatology, 25(1), 56.
5. OECD/European Observatory on Health Systems and Policies (2017), Romania: Country Health Profile 2017, State of Health in the EU,OECD Publishing, Paris/European Observatory on Health Systems and Policies, Brussels. http://dx.doi.org/10.1787/9789264283534-en
 Liver cancer occurs when normal liver cells begin to gr
Liver cancer occurs when normal liver cells begin to gr
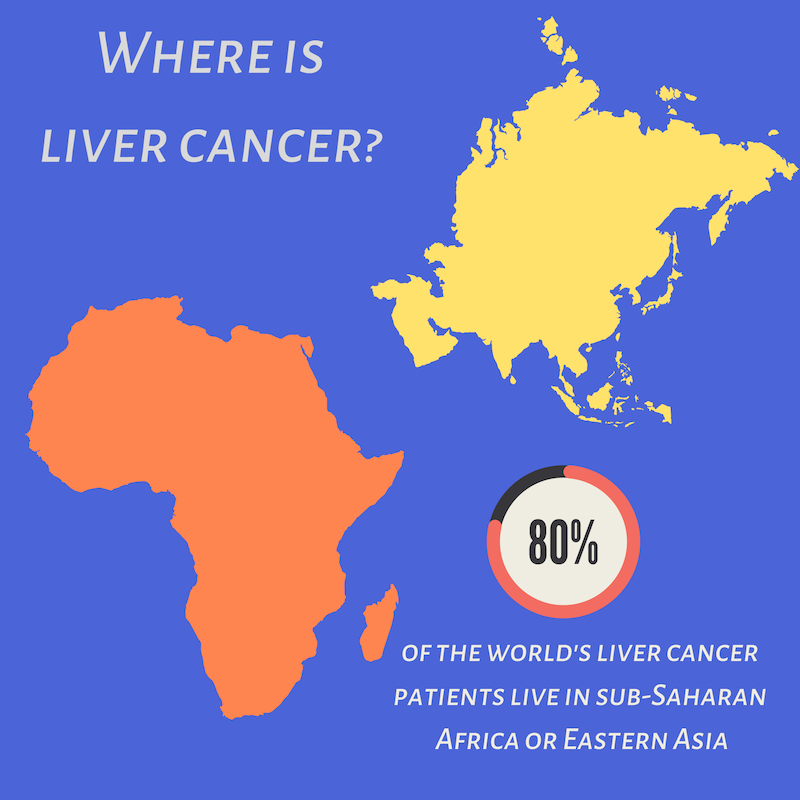
 October is Liver Cancer Awareness Month. Often we neglect to think about the link between hepatitis and liver cancer. Tuesday, Oct. 16, representatives from
October is Liver Cancer Awareness Month. Often we neglect to think about the link between hepatitis and liver cancer. Tuesday, Oct. 16, representatives from 

 Arizona’s hepatitis B story
Arizona’s hepatitis B story 
 Layal Rabat is a third culture kid who has spent years practicing the fine art of parachuting into projects as the need for her skills arises. She takes an intersectional approach to her work and does not shy away from any cause where injustice is present and her contribution is welcomed and necessary. Her experience lies in project management, traditional and digital communications using all mediums from her own voice to videos to writing to tweeting, assembling audience-specific information for delivery in an infinite amount of ways. An infinitely curious researcher and an obsessive collector and assembler of information, she is often seen playing a supportive role in the background and amplifying the voices of those directly affected by injustice in her community. Fluent in English & Arabic, intermediate in Spanish & knows a tiny bit of Armenian. Current issues are immigrant rights and public health. With a BS in Psychology & an MA in Social Justice & Human Rights, she is currently working as the Empowerment & Advocacy Manager at the Asian Pacific Community in Action, and volunteering her time as IT/Web & Social Media Coordinator at Phoenix Allies for Community Health. She also volunteers with the Restoration Project, Phoenix, and serves as a board member with Sonoran Prevention Works. In her spare time, she enjoys listening to music (& karaoke), reading, writing, photography, and traveling.
Layal Rabat is a third culture kid who has spent years practicing the fine art of parachuting into projects as the need for her skills arises. She takes an intersectional approach to her work and does not shy away from any cause where injustice is present and her contribution is welcomed and necessary. Her experience lies in project management, traditional and digital communications using all mediums from her own voice to videos to writing to tweeting, assembling audience-specific information for delivery in an infinite amount of ways. An infinitely curious researcher and an obsessive collector and assembler of information, she is often seen playing a supportive role in the background and amplifying the voices of those directly affected by injustice in her community. Fluent in English & Arabic, intermediate in Spanish & knows a tiny bit of Armenian. Current issues are immigrant rights and public health. With a BS in Psychology & an MA in Social Justice & Human Rights, she is currently working as the Empowerment & Advocacy Manager at the Asian Pacific Community in Action, and volunteering her time as IT/Web & Social Media Coordinator at Phoenix Allies for Community Health. She also volunteers with the Restoration Project, Phoenix, and serves as a board member with Sonoran Prevention Works. In her spare time, she enjoys listening to music (& karaoke), reading, writing, photography, and traveling. Access (AFIA) program at the Multicultural Aids Coalition (MAC), the Coalition Against Hepatitis for People of African Origin (CHIPO), the New England AIDS Education and Training Center (NEAETC), and the Harvard University Center for AIDS Research (CFAR) in continuing the national fight for federal recognition of National African Immigrant and Refugee HIV and Hepatitis Awareness Day (NAIRAHHA).
Access (AFIA) program at the Multicultural Aids Coalition (MAC), the Coalition Against Hepatitis for People of African Origin (CHIPO), the New England AIDS Education and Training Center (NEAETC), and the Harvard University Center for AIDS Research (CFAR) in continuing the national fight for federal recognition of National African Immigrant and Refugee HIV and Hepatitis Awareness Day (NAIRAHHA).



