Aroha Kawai just started a new job as amedical interpreter forPacific Islander patients diagnosed with COVID-19.As a critical source of communication for the providers and the patients, she is often called to work night and weekend shifts.Aroha had a difficult conversation with the family members of a critical COVID-19 patient on whether they should discontinue ventilation support for the ailing grandmother. During this time, Aroha’s family noticed changes in her behavior. She stopped eating regularly, lost weight and repeatedly cancelled plans to go out. Aroha dismissed her family’s concerns as physical manifestations of the emotional burnout from work.
Recently she attended a health fair hosted by her department at work. She approached a viral hepatitis screening booth and decided to get tested for hepatitis B. The following week, she received her results in the mail. Her results indicated that she had tested positive for hepatitis B. She shared her diagnosis with her mother who informed her that her grandfather died from liver cancer.
Aroha then followed up with her primary care doctor. She discovered that she had chronic hepatitis B. Even though the ultrasound did not show any evidence of cirrhosis, her doctor ordered an imaging test (U/S, CT, MRI) to screen for liver cancer. Unfortunately, Aroha was diagnosed with early-stageliver cancer.
Fortunately, the cancer had not spread and did not infect nearby blood vessels. Her doctor suggested a partial hepatectomy to remove the tumor safely as the rest of the liver was still healthy. Aroha decided to adhere to her doctor’s advice and successfully underwent the surgery. She has taken some time off from work to focus on recuperating from the surgery and spending time with loved ones.
The Challenge:
Dismissal of Symptoms:
Aroha initially ignored the physical symptoms of liver cancer. It is true that signs and symptoms may not necessarily be present.
However, it is crucial to take care of one’s health and never ignore warning signs. Fatigue, unintended weight loss, and loss of appetite are a few of the symptoms of liver cancer.
Cancer without Cirrhosis:
It is possible to get liver cancer without cirrhosis. Therefore, it is always important to screen for liver cancer if you have chronic hepatitis B infection.
Importance of Screening
Liver cancer screening is a highly effective method to detect malignant tumors and prevent cancer for those living with hepatitis B.
Early intervention increases the survival rate significantly and stops the cancer from spreading to other vital organs.
What can you do?
Get Help!
If you experience pain or discomfort of any kind, it is important to reach out for help. Set up an appointment with your doctor and discuss your concerns.
There is a good chance you might be misunderstanding an important health issue for side effects of stress or emotional burnout. Do not ignore your symptoms or feelings.
Get Screened!
Hepatitis B is a leading cause of liver cancer, most of the time it is because someone did not know they were infected with hepatitis B or were not managing their hepatitis B infection.
Everyone should be tested for hepatitis B to know their status. Ask your doctor for a hepatitis B screening today.
Stay on track!
If you have hepatitis B, it is critical to manage the progression of the virus in your liver. For this reason, it is important to go through liver cancer surveillance regularly. Discuss with your doctor if you are at high-risk and how often you should get screened.
It is recommended to get an ultrasound with blood work every 6 months to check how the virus is impacting the liver. This includes the alpha-fetoprotein (AFP) blood test to measure the levels of AFP in your blood as it may indicate the presence of cancer cells in your liver. This can also help detect any scarring or tumors.
What’s the Difference?: Herbal Remedies and Supplements vs. Western Medicine
Around the world, people consider the use of herbal remedies or supplements as a natural treatment for hepatitis B and/or D infection. These natural remedies have historically been advertised to boost the immune system and improve liver health. Herbal remedies or supplements are described as products made from botanicals or plants used to treat diseases and maintain health. They can be produced in a variety of forms including liquid extracts, teas, tablets/capsules, bath salts, oils, and ointments4.
Why do people choose to use herbal remedies?
The use of these products over time has social-cultural influences related to the distrust of and unfamiliarity with western medicine for management of hepatitis B or D infection. While herbal remedies have been used widely across cultures and contexts, patterns of racism, medical mistreatment, and inadequate delivery of care in western medicine have influenced the present state of treatment practices. In response to these barriers to sensitive and effective health care delivery, many groups such as Hmong and African communities often rely on herbal remedies and supplements to treat medical conditions and ease suffering.
Silymarin, milk thistle, and Kampo medicine
The distrust of western medicine has contributed to more widespread use of supplements such as silymarin (milk thistle) and Kampo medicine, as alternatives to manage hepatitis B or D infection. Many people believe that Silymarin can improve liver health through its antioxidant and free radical-fighting properties. Traditional Kampo medicine has been used for over 2,000 years to treat a variety of diseases including hepatitis B. One herbal treatment that is frequently used is bupleurum which many people believe can protect the liver or heal liver damage. Despite possible liver health benefits, neither supplement is a treatment for hepatitis B or D and may sometimes cause further harm to the liver4. It is important to note that there is presently no cure for hepatitis B.
False claims and bad interactions
Additionally, several alternative medicine companies often make false claims and testimonials to convince people to purchase expensive alternative treatments with false promises that are not based on scientific evidence. Herbal remedies and supplements may also interact with certain medications prescribed for those with hepatitis B and D, so it is important to seek the advice of a health care professional before use of any of these products3,4.
Strides in western health care
The long-standing hesitancy to participate in western health care is well-reasoned and firmly rooted in past wrongdoing on the part of often fundamentally racist institutions. While the western health care system remains far from perfect, it is important to remember that many strides continue to be made to correct the misdeeds of the past, and conversations around health equity and the social determinants of health (including racism) are becoming more and more common. Meanwhile, research has found that beliefs and misconceptions around western medicine can delay care and increase morbidity rates of hepatitis B in high-risk communities2.
It is vital for those living with hepatitis B or D to stay informed with scientific knowledge about supplements and herbal treatments to ensure these products are effective and safe in their daily life. The coordination of hepatitis B and D care by providers must do better to support those impacted by the viruses, in a way that is culturally sensitive and not dismissive of the harm that has been inflicted on communities of color and immigrant communities, who are more likely to be affected by hepatitis B and D1. Health care professionals and other service providers must continually work to improve their cultural humility. In addition, health care institutions practicing western medicine must work harder to ensure care is equitable and safe, and to center the voices, stories, and insights of community members in their work to repair the impacts of structural racism and medical mistreatment that have caused such deep distrust in western medical treatments.
To learn more about effective hepatitis B and D medications, check out our Drug Watch page!
Disclaimer: Herbal products are not U.S. FDA-approved, and the Hepatitis B Foundation cannot endorse the usage of such products that lack regulation and scientific evidence to deem them both effective and safe.
References
El-Serag, H., McGlynn, K. A., Graham, G. N., So, S., Howell, C. D., Fang, T., … & Thiel, T. K. (2010). Achieving health equity to eliminate racial, ethnic, and socioeconomic disparities in HBV-and HCV-associated liver disease. The Journal of Family Practice, 59(4 Suppl), S37.
Mukhtar, N. A., Evon, D. M., Yim, C., Lok, A. S., Lisha, N., Lisker-Melman, M., … & Khalili, M. (2021). Patient knowledge, beliefs and barriers to hepatitis B Care: results of a multicenter, multiethnic patient survey. Digestive diseases and sciences, 66(2), 434-441.
Globally, almost 300 million people are living with hepatitis B. Of these 300 million people, the highest burden is in the WHO Western Pacific region and WHO African region with 116 million people and 81 million people living with hepatitis B. 60 million people are infected in the WHO Eastern Mediterranean Region, 18 million in the WHO South-East Asia Region, 14 million in the WHO European Region and 5 million in the WHO Region of the Americas.1
Of these estimated 300 million people living with hepatitis B, only 10% were diagnosed, and of those who were diagnosed, only 22% of individuals eligible for treatment received antiviral therapies.2 Moreover, only 2% of Africans living with chronic hepatitis B infection receive a diagnosis and of those individuals, 0.1% receive treatment.3
So why aren’t people living with hepatitis B on treatment? Cost can be a barrier.
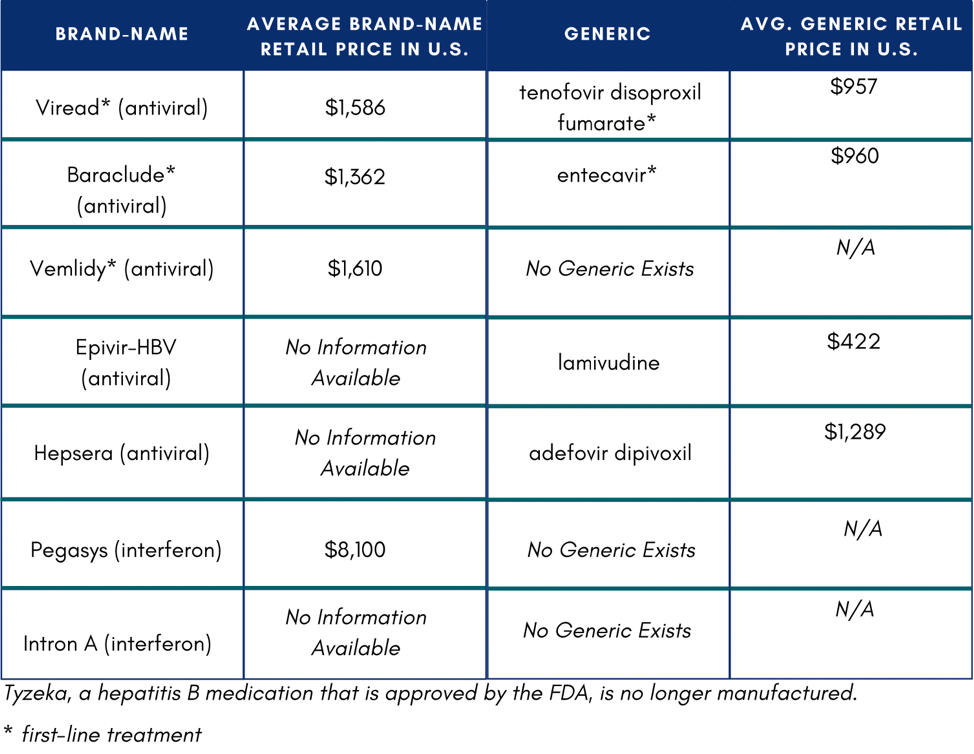
The Hepatitis B Foundation compiled a list of hepatitis B medications and their costs for a 30-day supply in the U.S.
In the U.S., if someone does not have insurance or know how to access Medicaid or Medicare, they might not be able to afford medication. If they were to pay out of pocket, medication would total $11,484 on the low end of costs.4 One study reported that low household income and publicly funded health insurance were negatively associated with willingness to accept hepatitis B treatment.5
The high cost of hepatitis B management was found to be a barrier in a research study in Ghana. This study found that a typical cost of hepatitis B medication (Tenofovir), was Ghc 3600, or $670 USD annually.6 The average income is about Ghc 9,600 or $1,778 – this means the cost of hepatitis B medication would be about 38% of an average Ghanaian income.6
Another study in Burkina Faso found that cost was a barrier to access to treatment. For someone living with hepatitis B, the total cost for a full diagnosis is estimated to be $209 USD, when in 2020,5 33.7% of the population lived on less than $1.90 a day and the gross national income per capita in 2014 was $700.7 For the treatment itself, the study found that it cost $54 a year for tenofovir and $23 a year for lamivudine. One individual reported that they had to stop treatment because of the cost.6
What can be done to help with cost for hepatitis B treatment?
In the U.S., there are patient assistance programs that can help alleviate costs for some people. These special prices are offered by online pharmacies, co-pay assistance cards, or pharmaceutical companies. DiRx, a new online pharmacy, has added two front-line medications for chronic hepatitis B infection – generic Viread® (Tenofovir) and generic Baraclude® (Entecavir) – and will be offering the medications at greatly discounted prices. Specifically, 30-count supplies of Entecavir will be $33, and Tenofovir $21, compared to the average retail price of $1,188. To access Tenofovir or Entecavir at discounted prices, patients should visit DiRxHealth.com and use promo code HBFSAVE. Any hepatitis B patient with a valid U.S. prescription will be able to order and benefit from free U.S. shipping, with no pre-qualifications and health insurance required. RxOutreach is another online pharmacy that provides reduced cost tenofovir and entecavir, and recently had a special offer for free medication for up to 12-months. For people in the U.S. taking Vemlidy, Gilead offers a patient assistance program for those who meet certain criteria. Patient Advocate Foundation and Prescription Hope offer co-pay assistance programs for eligible individuals with insurance who cannot afford their insurance co-pays.
We must continue to bring awareness to hepatitis B. Through advocacy and continued discussion, we can improve political and government will which is most important for access to education, prevention, testing, and treatment of hepatitis B. Currently, hepatitis B is not included in The Global Fund To Fight HIV, Tuberculosis, and Malaria which offers countries like Burkina Faso and Ghana free treatment for these three diseases. We can advocate for hepatitis B to be included in this program or a viral hepatitis program like this which would help eliminate hepatitis B. Moreover, countries can use existing HIV infrastructure and incorporate hepatitis B into that space. Through cross organizational collaboration, advocacy, increasing education, and improving advocacy this can be accomplished.
The Hepatitis B Foundation is dedicated to accomplishing these efforts. We published Health Insurance Costs Impacting Shoppers Living with Hepatitis B – a comprehensive report that details our findings from analyzing 2019 and 2020 silver-level health insurance plans for potential discriminatory tiering of hepatitis B treatments. The report contains a list of things to consider when choosing health insurance plans, trends that may drive up the cost of treatment, and an overview of health insurance companies that displayed discriminatory practices. You can use the information on our site to help advocate for yourself, report your experience with discrimination on the Hepatitis B Foundation’s Discrimination Registry, or contact the Hepatitis B Foundation at discrimination@hepb.org.
Web Annex 1. Key data at a glance. In: Global progress report on HIV, viral hepatitis and sexually transmitted infections, 2021. Accountability for the global health sector strategies 2016–2021: actions for impact. Geneva: World Health Organization; 2021. Licence: CC BY-NC-SA 3.0 IGO.
Polaris Observatory Collaborators (2018). Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: a modelling study. The lancet. Gastroenterology & hepatology, 3(6), 383–403. https://doi.org/10.1016/S2468-1253(18)30056-6
Adjei CA, Stutterheim SE, Naab F, Ruiter RAC (2019) Barriers to chronic Hepatitis B treatment and care in Ghana: A qualitative study with people with Hepatitis B and healthcare providers. PLoS ONE 14(12): e0225830. https://doi.org/10.1371/journal.pone.0225830
Mukhtar, N. A., Evon, D. M., Yim, C., Lok, A. S., Lisha, N., Lisker-Melman, M., Hassan, M., Janssen, H., & Khalili, M. (2021). Patient Knowledge, Beliefs and Barriers to Hepatitis B Care: Results of a Multicenter, Multiethnic Patient Survey. Digestive diseases and sciences, 66(2), 434–441. https://doi.org/10.1007/s10620-020-06224-3
Giles-Vernick, T., Hejoaka, F., Sanou, A., Shimakawa, Y., Bamba, I., & Traoré, A. (2016). Barriers to Linkage to Care for Hepatitis B Virus Infection: A Qualitative Analysis in Burkina Faso, West Africa. The American journal of tropical medicine and hygiene, 95(6), 1368–1375. https://doi.org/10.4269/ajtmh.16-0398
The company GlaxoSmithKline (GSK) is launching a new clinical trial, called B-Together, that will investigate how two study drugs might work together to treat chronic hepatitis B (CHB). Researchers are hoping to find new potential treatments that could be more effective than those that are currently available and could lead to positive results that last long after the treatment ends. Participants in this trial could play a role in shaping science and changing the landscape of CHB treatment around the world, and will have an opportunity to learn more about the disease itself.
The two drugs that will be investigated in this trial are GSK3228836 and pegylated interferon, also known as Pegasys. In a previous Phase 2 trial, people living with CHB received GSK3228836 for 4 weeks. The Phase 2b B-Together trial will test longer treatment with GSK3228836, followed by Pegasys, to see what effects this may have on viral antigens (such as HBsAg) in the body.
About the Study Drugs
GSK3228836 is an investigational drug being tested as a potential treatment for CHB, meaning it is not yet approved for this purpose. Current medicines available to treat CHB only stop the virus from multiplying – they do not enable the body to fully clear the infection, so people have to keep taking these medicines. GSK3228836 is designed to stop the virus from producing proteins that may prevent the immune system from fighting the virus. Thus, the study drug may potentially allow the body to gain control over the infection.
The other drug used in this study, Pegasys, is a medicine that is already used on its own by doctors to treat CHB. Pegasys works by enhancing the body’s immune response to viral infections such as hepatitis B.
What Will Happen During This Trial?
During this trial, all participants will receive GSK3228836 followed by Pegasys. After you have finished treatment with GSK3228836, your doctor will check if it is appropriate for you to start treatment with Pegasys. If it is not appropriate, you may not receive Pegasys at all. At the beginning of the trial, you will be assigned by chance to one of two groups. Each group will receive the study drugs for different lengths of time. You will know which group you are in. The B-Together trial lasts about 79 weeks for each participant. This includes a screening period, a study treatment period, and a follow-up period.
Screening Period
At a screening visit, the study doctor will give you a physical examination, ask about your medical history, and conduct medical tests. The screening period may last up to about 6.5 weeks while the study doctor reviews the results of your screening visit to determine if you meet all requirements for participation.
Trial Treatment period
While receiving GSK3228836, you will visit the clinic for either 12 or 24 weeks. For the first two weeks of your treatment with GSK3228836, you will visit twice per week and for the remaining weeks you will visit the clinic once per week.
When you have finished treatment with GSK3228836, your doctor will assess if it is appropriate for you to start treatment with Pegasys. If it is appropriate, then you will then receive treatment with Pegasys once a week for up to 24 weeks.
In some countries, it will be possible for you to self-inject Pegasys at home after discussion and training from your study doctor. This could reduce the number of times you have to visit the clinic.
Other study activities will vary from visit to visit and may include:
Discussions about your health and medications you may take outside the trial
Measurement of vital signs (i.e. blood pressure, pulse, weight)
Collection of blood or urine samples
Physical examination
Questionnaires about your health and well-being
Follow-Up Period
During the 24-week follow-up period, you will not receive injections of study treatment, but you will complete other study visit activities as scheduled. There are eight visits scheduled in the follow up period. Your study participation will end about 72 weeks after your first dose of the trial drug.
Who Can Participate?
You may be eligible to participate in this trial if you are at least 18 years old, have been living with documented CHB for at least six months, and have also been receiving stable nucleos(t)ide treatment (not telbivudine) with no changes for at least six months prior to screening and no planned changes for the duration of the study. There are other eligibility requirements that the study doctor will review with you. Individuals who have a current co-infection with or past history of hepatitis C virus, HIV or hepatitis D virus are not eligible to participate in this trial.
Where Is This Trial Taking Place?
This trial is ongoing in the UK, Spain, Russia, Poland, Italy, Korea, Japan, China, the US, Canada, and South Africa.
You can play a role in shaping your own health and the science of tomorrow! To learn more about this trial and check your eligibility to participate, visit https://clinicaltrials.gov/ct2/show/NCT04676724.
If you have chronic hepatitis B or are newly diagnosed, it’s important to see a medical provider who has experience managing and treating hepatitis B.
Having a medical provider with hepatitis B expertise on your team not only safeguards your health but also lessens the stress of having a chronic liver disease. “My specialist gave me all the possible scenarios, but most importantly, he gave me my life back,” one hepatitis B patient recalled.
When first diagnosed, it’s often a primary health provider (PCP) or for children a pediatrician who orders diagnostic tests for hepatitis B. Doctors may run additional blood tests and/or immediately refer you to a liver specialist. If your PCP has experience managing and treating hepatitis B, you may decide to continue your hepatitis B care with that provider. Or, they may recommend a specialist who accepts your insurance or practices in the same healthcare system. But, you may have to do some research to find the best specialist to treat your hepatitis B.
There are two types of specialists who treat liver diseases:
A gastroenterologist is an internist who has trained in digestive disorders including the liver, but how much liver expertise a gastroenterologist (GI doctor) has varies based on their training. It’s important to find out if they specialize in liver diseases and if they have experience with hepatitis B.
A hepatologist is a physician who specializes in the liver. This doctor has the most expertise and should be up-to-date about new treatments and clinical trials. But not all hepatologists have treated hepatitis B. Many will have treated hepatitis C, but not hepatitis B, so you need to ask.
Tips for finding a specialist:
Are they in the Hepatitis B Foundation directory? The Foundation has a Physician Directory of medical providers who treat hepatitis B around the world. These doctors have voluntarily signed upto be included in the database. It is not an exhaustive list, there may be hepatitis B specialists in your area who have not yet joined the directory.
Call the practice ahead of time and ask questions. How many hepatitis B patients have they treated? Do they participate in any clinical trials? Are they aware of current monitoring and treatment guidelines for hepatitis B?
What’s the doctor’s reputation? Does anyone in your community see a liver specialist for viral hepatitis? Whom do they recommend?
Will you actually see the specialist or an assistant? Do you see a specialist only if there is a need for treatment? If you go to a teaching hospital, do you see the doctor or an intern, fellow or resident?
You are entering into a long-term relationship with someone who may care for you for many years. You need their expertise, but you also need to feel comfortable working with them. Do they listen when you speak and make eye contact? Trust and rapport are very critical.
“It’s really important that they don’t judge me,” one hepatitis B patient explained. Another patient said that finding a doctor who spoke his language, or had an assistant who was fluent in his language, helped immensely.
Once you identify a specialist, here are some questions to ask:
Is the specialist accepting new patients? How long do you have to wait to get an appointment?
What hospital or lab do they use, and are they convenient for you? It’s important for you to always use the same lab so you have consistent results that allow apples-to-apples comparisons.
Will the doctor call you with the results or will a nurse or other assistants communicate with you?
What would you like your care plan to be? Will you go for blood tests and then see the specialist? Typically, hepatitis B patients get blood tests once or twice a year to monitor their liver, unless they are undergoing treatment.
How to design a long-distance care plan if the specialist is far away: Sometimes, the best hepatitis B specialist is a few hours drive from where you live, but distance doesn’t have to be a deal-breaker. Many people see a specialist for a first visit, and afterwards, simply have their PCPs or local labs email lab results to the specialist. For this remote healthcare relationship to work, your PCP needs to be willing to partner with the specialist. Also, your specialist needs to be open to telephone or video consultations with you as needed.
Technology matters. Sharing medical records and lab tests electronically make a remote relationship work smoothly. If there are firewalls between practices, find out how to ensure your PCP and specialist share your medical records. Be prepared, you may have to be the conduit if the two healthcare systems don’t talk to each other.
Insurance and cost: Ideally, the hepatitis B specialist closest to you accepts your insurance or is in your provider network. That doesn’t always happen so finding out the charges in advance is important.
Will the specialist bill your insurance or will you need to pay the fee upfront and manage the insurance reimbursement yourself?
How much do you have to pay out-of-pocket if the specialist is outside your network, or if you are not insured? Some specialists charge a lower fee to uninsured patients. You may be able to have an annual consultation with a specialist and bring your lab results.
One hepatitis B patient reported he was not entirely happy with the specialist his PCP referred him to. “At the time, I had great insurance so all the tests he ordered weren’t a lot of money out-of-pocket,” he said. “But then I changed jobs and I couldn’t afford all of his tests, and he wanted me to go on treatment though my lab reports didn’t justify it.
“I went looking for a new one and found one in the Hepatitis B Foundation’s website,” he said. “I had to drive farther to see him, but his knowledge and patience were very comforting and he spoke my primary language. He really helped me regain confidence in life.”
Prepare for your visit: Before you see your hepatitis B medical provider, put together a list of questions (see sample questions) and have your lab reports available — either bring hard copies or call ahead of time to make sure the doctor has access to your latest labs and medical records.
After you meet with your specialist, take some time to reflect. Are you happy with the doctor? Did he or she communicate well? Are you clear about what you need to do in the weeks and months ahead to take charge of your health? If the answer is yes, congratulations, you have assembled a good healthcare team.
Are you a member of the African diaspora in the United States? Do you work for an organization that serves these communities? We would love for you to join CHIPO – the Coalition Against Hepatitis for People of African Origin! CHIPO is a national community coalition, co-founded and led by the Hepatitis B Foundation. Our members include a variety of individuals and organizations from all over the country, who are interested in and focused on addressing the high rates of hepatitis B among African communities in the US., which are disproportionately affected by hepatitis B and liver cancer. In some parts of the country, rates of chronic hepatitis B infection in African communities are estimated to range between 5 and 15% of people.
The purpose of CHIPO is to provide a space for an open exchange of ideas, best practices, and information about how to dismantle some of the many barriers that stand in the way of preventing, diagnosing, and treating chronic hepatitis B infection, and preventing liver cancer, in African immigrant communities. These barriers include a lack of disease awareness, high rates of stigma, limited access to healthcare and services, and the silent nature of the disease, which often does not present any symptoms until significant liver damage has occurred – a process which could take years or even decades. As a result, most African community members who have hepatitis B DO NOT KNOW that they are infected. This puts them at much greater risk for premature death from cirrhosis or liver cancer.
CHIPO, meaning “gift” in the Shona language, aims to disseminate accurate information about hepatitis B transmission, prevention, and treatment among community members, healthcare providers, and organizational leaders, and to improve the national capacity to raise hepatitis B awareness, testing, vaccination, and linkage to care among highly affected African communities. CHIPO also works to ensure that African immigrant communities are represented in HBV discussions and programs regionally and nationally. This is achieved through advocacy and the development of national and local partnerships. We currently have over 35 coalition partners around the U.S., dedicated to addressing viral hepatitis in African communities.
The activities of CHIPO are many and diverse. They include bimonthly virtual meetings, which often center around a presentation by a coalition member about measures or interventions that have been undertaken or research that has been done to achieve one of CHIPO’s objectives – namely improving awareness about and access to hepatitis B information, screening, vaccination, and linkage to follow-up care. Other activities include educational community events and presentations; supporting the design and implementation of initiatives to help accomplish CHIPO’s goals, such as the CDC Know Hepatitis B campaign (discussed below) and a recent grant from Bristol Myers Squibb to raise awareness about liver cancer and understanding about the link between hepatitis B and liver cancer in African immigrant communities; and promoting the work of coalition members locally and nationwide.
An example of a project for which CHIPO provided great support and guidance was the production of the first nationally available hepatitis B educational resources, specifically for African populations. Created in collaboration with the Centers for Disease Control and Prevention (CDC), these materials are part of a train-the-trainer-based model, and include a suite of materials, including a downloadable presentation on hepatitis B for community health workers, a printable flip chart for direct community education, and supporting fact sheets and resources. The presentation and flip chart have also been translated into Amharic, Arabic, French, and Swahili.
To read more about CHIPO, including previous blog posts, articles, and meeting minutes, and to access a full list of our members and the work they are doing around the country, visit our website.
Does this work sound interesting to you? Would you like to work with us to achieve lower rates of hepatitis B and liver cancer in African immigrant communities through increasing awareness, screening, vaccination, and linkage to care? Join us! Anyone is welcome to join CHIPO – contact the coordinator to get involved. We hope to see you on our next call!
On Monday September 21st, a virtual celebration was held in honor of the sixth anniversary of National African Immigrant and Refugee HIV and Hepatitis Awareness (NAIRHHA) Day. This day, which itself is commemorated on September 9th, was created to build awareness and dismantle stigma around HIV and viral hepatitis in African immigrant and refugee communities. It takes place in September because this is the month that has been designated as National African Immigrant Month (NAIM) in the United States to celebrate the diverse and remarkable contributions African immigrants have made to enrich the United States, in spheres ranging from sports to writing to politics.
The virtual celebration that occurred last Monday included a discussion of the history of NAIRHHA Day and how it came to exist in its present form, a conversation with a hepatitis B advocate who is living with the disease, discourse about the importance of NAIRHHA Day on the national level and implications for making it a federally recognized day, and trivia questions about HIV and hepatitis B.
History of NAIRHHA Day: The Journey from 2014 to Present
Moderator: Chioma Nnaji, MPH, MEd, Program Director, Multicultural AIDS Coalition
Panelists: Augustus Woyah, Program Officer for Minority AIDS Initiative, Maryland Department of Health
Amanda Lugg, Director of Advocacy and LGBTQ Programming, African Services Committee
The idea for NAIRHHA Day was first conceived in 2006 at a convening of the Ethiopian Community Development Corporation in Washington, DC, at a session sponsored by Office of Minority Health about HIV in African immigrant communities. Conferences started to occur, primarily in the Northeast, although there was also interest in Atlanta and Seattle. It seemed that an opportunity had finally become available for advocates, researchers, and providers to all come together and focus on data collection, community mobilization, and policy work around HIV and viral hepatitis in African immigrant communities. The African National HIV/AIDS Alliance was established in 2010 and awareness days started in 2012 (Augustus played a large role in this). In 2014, Chioma Nnaji became connected to Sylvie Bello, the Executive Director of the Cameroonian Association in Washington, DC, and they, along with Amanda and Augustus, worked to get NAIRHHA Day off the ground. Chioma has largely spearheaded efforts to have NAIRHHA Day recognized nationally.
In terms of some of the challenges that have and continue to exist around NAIRHHA Day, obtaining community leadership and organizational buy-in, as well as national attention, are at the forefront. Social media and other digital platforms have been widely used in order to amplify the cause and try to obtain federal recognition. Additionally, maintaining relationships with government agencies has been quite difficult and has become a clash of visions of sorts. There is a strong belief that NAIRHHA Day should be a community-driven effort, but government agencies often have their own priorities, which can be distinct from those of the community and grassroots organizers. This is not to discount the government and organizational partners that are still involved, however, including NASTAD, the Hepatitis B Foundation, CHIPO, CHIPO-NYC, and Africans for Improved Access at the Multicultural AIDS Coalition. Another challenge has been reinforcing the distinction between African immigrant and African American communities and not treating the Black community as a monolith. Drawing this distinction in both data and policy remains difficult, thus often rendering African immigrant communities invisible.
When pondering what areas could use improvement going forward, a number of different items were considered. These included incorporating COVID-19 into the conversation, along with viral hepatitis and HIV; addressing social and environmental determinants of health that lead to the over-prevalence of both infectious and non-communicable diseases in minority, and particularly African immigrant communities; adhering to the primary goal of community mobilization and including advocates and researchers to influence policy that provides linguistically and culturally appropriate services that address the most pressing issue of stigma; securing national attention; and obtaining resources. It is critical to remember that advocacy never ends, the need to magnify work and amplify voices is always present, there is no room for complacency, and there exists intersectionality in all issues (social and health justice are all-encompassing).
#justB Storyteller Interactive Discussion
Moderator: Farma Pene, Community Projects Coordinator in Viral Hepatitis Program, New York City Department of Health & Mental Hygiene
#justB Storyteller: Bright Ansah
In this session, Bright spoke about his experience with living with hepatitis B, including his diagnosis, treatment, and communication with his family. He spoke about being able to put a face to hepatitis B, which has helped many people and also allowed him to build strong relationships with a broader community. Bright found out about his status in 2014 and initially felt very lost. The first couple of years were a big struggle, as he did not want to worry his family and it took a while for him to come to peace with his diagnosis. This peace eventually came from a lot of extensive research, after which he found out that hepatitis B is not a death sentence and can be managed very well. He then started to think about what he could do to prevent someone else from becoming “a statistic.”
When asked what message he would share with newly diagnosed people, Bright stated that stress and anxiety are normal, but you are not alone. Every day, people find out they are infected. Bright has given his contact information to many different people and he emphasized the incredible importance of having a support system in place. When asked about how he overcame stigma and barriers, Bright replied that the biggest barrier is the mental hurdle. It took him about two years to not feel overwhelmed. Bright does still struggle with feeling rejected from clinical trials and finds this very frustrating – he still feels like he is being punished for having chronic hepatitis B.
The best advice that Bright can offer is to always be your own advocate and do your own research. If the first doctor or liver specialist that you find does not take you seriously or you feel that they are not doing enough for you, you do not need to stay with them and you can absolutely find another doctor. Bright went through this process himself and eventually found a doctor he likes at Johns Hopkins, through a friend of his. This can be a challenge with language barriers, but there are organizations that can help and there is a Specialist Directory tool on the Hepatitis B Foundation website, a resource that Bright stated he found very helpful, along with the website of the National Institutes of Health (NIH). Farma reiterated that the HBF website is a great place to visit to understand lab results in plain language, and offers a good collection of resources for family and community members of people living with hepatitis B. Bright finds that the most important questions to ask are: What exactly is your status and viral load? What should reasonable expectations for your life and health be? Is treatment appropriate and if so, which one? It is crucial to establish mutual respect with your doctor, and to iterate what expectations you have for your doctor as well. The most important messages are: Reach out. Ask questions. Stand up for yourself. You are not alone.
The Important Role that NAIRHHA Day Plays from a National and Policy Prospective
Moderator: Chioma Nnaji, MPH, MEd, Program Director, Multicultural AIDS Coalition
Panelists: Boatemaa Ntiri-Reid, JD, MPH, Hepatitis Director, NASTAD
Jennease Hyatt, Community Liaison for Boston/New England, GILEAD
The final conversation focused on why NAIRHHA Day should become a nationally recognized holiday. VIral hepatitis is the seventh leading cause of death globally. Nineteen million African adults are living with hep C, and 5-8% are living with hep B. Hep B and HIV need to be considered part of the health portfolio of African immigrants, with care taken that this does not compound stigma. NAIRHHA Day is really an opportunity to focus on this community specifically. You get things done by doing them yourselves and we are who we’ve been waiting for.
There is a strong need for a multi-faceted approach to this work and for local, state, and national partnerships. African immigrants need to be at the forefront of the HIV/AIDS conversation. In Massachusetts specifically, over half of new HIV infections are in immigrant communities: These communities need to be leading the conversation. In terms of the role that government agencies play in NAIRHHA day, this needs to be more than a supportive role. We need to talk about novel approaches. We know that there are healthcare disparities. We need to consider how to use funding to build capacity and engagement, and make sure this work moves forward. This should include counting in community members and small businesses and bringing people to the table who are not usually there. The community really wants to be engaged. Promoting testing and awareness at soccer games, for example, is a great idea. We need strong partnerships and leadership from the beginning and to determine different approaches and thus different outcomes. Community members are the experts and we need to treat them as such.
Across the country, there are jurisdictions that have a prevalence of 40,000 people living with hepatitis in a state and viral hepatitis staff have teams of 1-7. Local and state health departments have more of a role to play. CDC publishes a list of viral hepatitis coordinators by state. It would be great to close the gap with them and discuss more about what they are doing generally and how to get them more involved in NAIRHHA Day specifically. In thinking about a vision for NAIRHHA Day next year, thoughts included that everyone who serves African immigrant communities (including health centers and multi-service organizations) needs to see themselves as part of the solution. Additionally, federal representation should be part of NAIRHHA Day next year.
Trivia and Conclusion
The event concluded with trivia questions about HIV and hepatitis B prevention, testing, and treatment. Amazing music was provided by DJ WhySham and Laura O (@LauraO_TV) served as an excellent moderator. Thanks to everyone who participated and we look forward to another wonderful event next year!
A common question among people living with hepatitis B and their families is, “What happened to the cure for hepatitis B?” You can find answers in a new commentary by Dr. Timothy Block, HBF president and co-founder; Dr. Chari Cohen, senior vice president; and Maureen Kamischke, our director of international engagement.
The Hepatitis B Foundation’s Commentaries on the Cure is a new series written by hepatitis B experts. The series will feature thoughts and updates about the progress being made towards a cure for hepatitis B. Many of you have been awaiting a cure for years, and we understand that the wait can be frustrating. In addition to providing a look into the drug development process, we hope this series will serve as a source of information and hope for individuals living with hepatitis B.
Over the last 10 years, great strides have been made in hepatitis B cure research. The number of therapies in clinical trial stages has more than doubled, and four potential treatments for hepatitis Delta are in development! We believe that at least a “functional” cure is on it’s way, but it is extremely difficult to predict when one will be available. According to the Pharmaceutical Research and Manufacturers of America, it takes an average of 12-15 years to bring a drug from research to market. New treatments must undergo a rigorous testing process to ensure that it is both safe and effective for a large population. This process is extremely expensive – costing around $800 million USD per drug – and can be influenced by numerous factors, such as the number of volunteers for a clinical trial.
In recent years, we have seen an increase in interest and investments in a cure for hepatitis B, but more funding and support are needed to complete the journey. The Hepatitis B Foundation will continue to give the hepatitis B community a platform to share their voice, and advocate for the resources needed for the cure.
The Hepatitis B Foundation is thrilled to announce the addition of a new clinical trials search tool to our website! People around the world can now easily search for clinical trial opportunities on the Hepatitis B Foundation website. Created by Antidote – a company that designs technologies to link patients with scientific opportunities – the new tool filters through all of the trials listed in the U.S. National Library of Medicine’s database of private and publicly funded studies. Searching for clinical trials can be time-consuming and confusing to navigate, but this resource eases the process by finding the best trials for you based upon a series of questions.
You can now search for hepatitis B, hepatitisD and liver cancerclinical trials with a few simple clicks! Clinical trials are a series of research phases that a new drug must go through in order to be approved for widespread use. They are an essential to proving that a treatment is safe and effective for the larger population. Generally, these trials take 10-15 years to go from the laboratory to the public, but delays in finding or retaining enough volunteers can extend the process.
Diverse participationinclinical trials is needed to make sure that a treatment is effective for all groups. Research diversity matters greatly for several reasons. Studies have shown that different races and ethnicities may respond differently to a certain medication. In addition, researchers need to examine the impact of the medication on the populations that will eventually use them. According to data from the U.S. Food and Drug Administration (US FDA), individuals from Africa and Asia or of African and Asian descent consistently remain underrepresented in clinical trials; these populations are also disproportionately impacted by hepatitis B. If these groups are underrepresented in trials for hepatitis B treatments, new drugs may not be as effective in these communities, or there may be side effects that researchers were not aware of.
How Our Clinical Trials Finder Works
Using our Clinical Trial Finder takes just a few minutes. After clicking the ‘search’ button, the user will answer a series of questions of general demographic and health questions to determine what trials are near you and you fit the criteria for. You will be able to view the available trials at any point while answering questions, but answering all of the questions will give you the best results. You will also have the option to leave your email to receive personalized trial alerts for new trials that you are eligible for in your area! The new tool is designed to match those who wish to join a clinical trial to the best option for them; it is not designed to benefit any company.
Benefits of Participating in Clinical Trials
While participating in clinical trials helps drug developers, it can also provide major benefits to the participant as well! Blood work, treatments, and monitoring – which can be expensive – are often provided for free to those who are eligible for the duration of their participation in the study. Volunteers can also potentially benefit from the latest medical advancements and developments!
Help Improve the Future of Clinical Trials
5You can also help improve the future of drug development and clinical trials by taking our patientengagement survey! The survey, which takes approximately 20-25 minutes to complete, will be made available for use by the US FDA and drug development researchers to help clinical trial development for future hepatitis B therapies. All survey responses are anonymous.
In January of 2020, the Centers for Medicare and Medicaid Services (CMS) proposed a new rule that could increase the out-of-pocket costs for people who take prescription medication for hepatitis B in the U.S. The proposed rule states that health insurance companies would be able to collect patient coinsurance through pharmaceutical manufacturer financial assistance. However, the insurance companies will be allowed to disregard any coinsurance paid with copay assistance when calculating how much the patient has paid toward their deductible and annual out-of-pocket (OOP) limit.
This proposal – titled 2021 Notice of Benefit and Payment Parameters – reverses a recent ruling that would have required health insurance companies to count the value of manufacturer copay assistance toward an enrollee’s annual deductible and OOP limit in most circumstances1. This rule acknowledged that manufacturer copay assistance helps lessen the financial burden of medications for patients. In the US, prescription drugs can be extremely costly, making manufacturer’s copay assistance programs necessary for many patients. For example, brand name treatments are often expensive in order to help pharmaceutical companies earn back the costs of the research and time spent making the medication. Sometimes, the brand name treatments are the only ones that are available, like Vemlidy, or the only version that a person can take. A reversal of the rule would mean that hepatitis B patients and those living with other chronic illnesses may have to pay a larger amount of out-of-pocket costs for their medications.
To understand the significance of this change, we first need to understand what a copay accumulator is.
What is a Copay Accumulator Program and How Does It Work?
A copay accumulator – or accumulator adjustment program – is a strategy used by insurance companies and Pharmacy BenefitsManagers (PBMs) that stop manufacturer copay assistance coupons from counting towards two things: 1) the deductible and 2) the maximum out-of-pocket spending. What does this mean?
Previously, a person could receive financial assistance from companies that make a drug, and that would count towards their deductible and/or out-of-pocket costs, depending upon the insurance plan. Pharmaceutical companies often provide financial assistance (such as a co-pay card) to help underinsured individuals afford expensive medications. This means that the person paying for the drug would end up saving money, often thousands of dollars.
Why Is This an Issue?
As the AIDS Institute explains it, “ … the trend in health insurance benefit design is to shift more of the cost of health care to patients through high deductibles and coinsurance rates …In order to afford the medicine they need, patients increasingly rely on manufacturer copay assistance.” With copay accumulators, the individuals who need assistance the most will be unable to receive it, and will end up paying more for their treatments.
As shown in the above image, with a copay accumulator program – meaning her manufacturer’s assistance is no longer counted toward her out-of-pocket limit- the consumer ends up paying more, while the insurance company is able to reduce the amount they are paying.
Copay accumulator programs are making life-saving treatments increasingly inaccessible. Research shows that the more out-of-pocket costs a person has to pay, the more likely they are to abandon their medication. Once on a hepatitis B medication, stopping suddenly or only taking it once in a while can cause flares and lead to an even higher risk of liver damage.
In the United States, many of those who are living with hepatitis B come from underserved populations with limited access to healthcare. Oftentimes, cultural differences and language barriers can make it difficult to access and utilize the services they need. Now, copay accumulators are making the navigation process even more complex and placing a higher cost burden on patients.
1The rule required insurance companies to count manufacturer copay assistance toward a patient’s deductible and OOP limit for all brand name drugs for which there is no generic alternative and in cases where the patient gained access to the brand name drug through an insurance plan’s appeals or exceptions process.







 In the U.S., if someone does not have insurance or know how to access Medicaid or Medicare, they might not be able to afford medication. If they were to pay out of pocket, medication would total $11,484 on the low end of costs.4 One study reported that low household income and publicly funded health insurance were negatively associated with willingness to accept hepatitis B treatment.5
In the U.S., if someone does not have insurance or know how to access Medicaid or Medicare, they might not be able to afford medication. If they were to pay out of pocket, medication would total $11,484 on the low end of costs.4 One study reported that low household income and publicly funded health insurance were negatively associated with willingness to accept hepatitis B treatment.5




 The Hepatitis B Foundation is thrilled to announce the addition of a new clinical trials search tool to our website! People around the world can now easily search for clinical trial opportunities on the Hepatitis B Foundation website. Created by Antidote – a company that designs technologies to link patients with scientific opportunities – the new tool filters through all of the trials listed in the U.S. National Library of Medicine’s database of private and publicly funded studies. Searching for clinical trials can be time-consuming and confusing to navigate, but this resource eases the process by finding the best trials for you based upon a series of questions.
The Hepatitis B Foundation is thrilled to announce the addition of a new clinical trials search tool to our website! People around the world can now easily search for clinical trial opportunities on the Hepatitis B Foundation website. Created by Antidote – a company that designs technologies to link patients with scientific opportunities – the new tool filters through all of the trials listed in the U.S. National Library of Medicine’s database of private and publicly funded studies. Searching for clinical trials can be time-consuming and confusing to navigate, but this resource eases the process by finding the best trials for you based upon a series of questions.