April 21st and 22nd, 2022 marked the occurrence of a roundtable meeting solely focused on hepatitis delta virus (HDV), which was jointly hosted by the American Liver Foundation and the Hepatitis B Foundation. This was one in a series of events taking place this year to raise the profile of hepatitis delta, a serious coinfection of hepatitis B virus (HBV) that is estimated to affect between 5 and 10% of people who are living with HBV. HDV is more severe than HBV alone, with a 70% chance of developing into cirrhosis or liver cancer if unmanaged, compared to an approximately 25% chance for those living with HBV alone. With approval of the first official treatment for hepatitis delta in Europe in July of 2020, expected approval in the United States later in 2022, and other treatments moving through the clinical trial pipeline, more is happening in the world of hepatitis delta than ever before. Despite the promising treatment landscape, the virus still remains significantly under-diagnosed (making estimation of true prevalence difficult), largely due to lack of awareness, low prioritization compared to other health conditions, and limited advocacy, and big questions persist about treatment equity, including access to knowledgeable providers, clinical trials, and available medications. The purpose of this roundtable was to begin a conversation among a diverse group of stakeholders about some of these issues, to bring attention to HDV and its potential consequences, to identify unmet needs in this area, and to prepare calls to action and next steps to address these needs.
Participants at the roundtable included individuals living with hepatitis delta, caregivers, healthcare providers, public health professionals, and representatives from community-based organizations. The conversation was very generative and really underscored some of the key issues that exist around hepatitis delta, including gaps in awareness and knowledge among medical and high-risk communities and limited access to and availability of HDV screening and care. These factors lead to under-diagnosis and under-surveillance, making the production of accurate data difficult, which in turn complicates advocacy efforts, since compelling data is often a key ingredient for policy change that might make screening, treatment, and linkage to care more available and accessible.
The ultimate planned outcome of this virtual event will be production of a white paper that will highlight key takeaways from the discussion, clearly outline unmet needs and priority issues for people living with HDV, and detail calls to action for stakeholders at every level to meet these needs and overcome some of the significant barriers and challenges that persist in diagnosing, managing, and treating HDV.
Another goal of the meeting was to begin to develop resources that can better support and engage the larger community around HDV awareness and advocacy – a first step toward this goal will be creation and dissemination of a visually appealing infographic, which will provide at-a-glance information about HDV and its estimated prevalence, transmission, prevention, testing, and treatment.
The white paper and infographic are expected to be complete by early summer 2022. The organizers of this roundtable meeting are hopeful that its outcomes will bring hepatitis delta virus more into focus for various stakeholder communities and generate more engagement and energy around this dangerous virus that has long been neglected and is not receiving the attention it deserves.
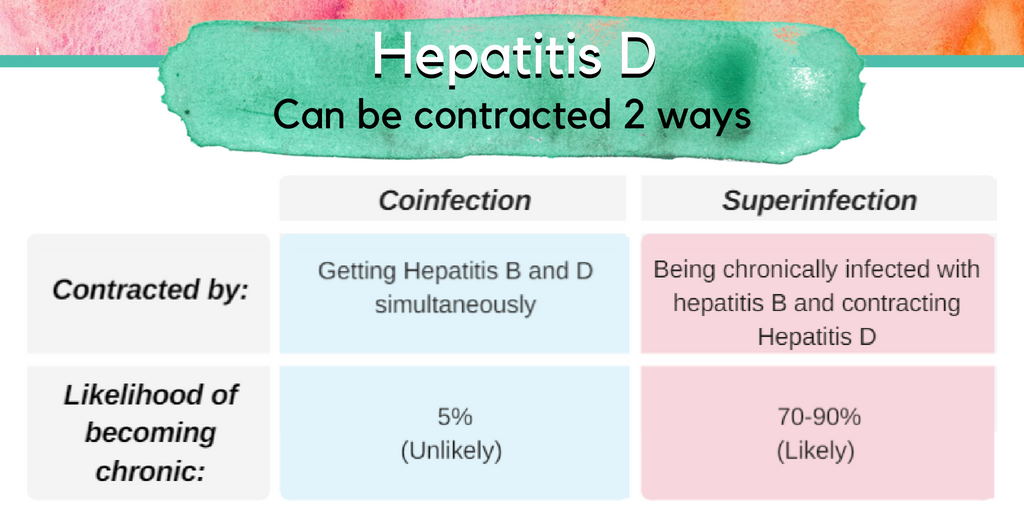
2022 is shaping up to be a big year for hepatitis delta, the rare but serious virus that can co-infect people who are already living with hepatitis B. As a quick refresher, hepatitis delta is a virus that depends upon the hepatitis B virus in order to survive and replicate – so only those who are already living with hepatitis B can become infected with hepatitis delta. Hepatitis delta virus (HDV) is believed to infect between 5 and 10% of people living with hepatitis B virus (HBV). HDV can occur through either a superinfection or a coinfection. A superinfection occurs when someone who is already living with HBV contracts HDV, in which case there is a very high chance that the individual will develop chronic (lifelong) infections of both HBV and HDV. A coinfection occurs when both HBV and HDV are contracted at the same time – when this happens in adults, both infections tend to clear within six months and there is only a 5% chance that chronic HBV and HDV will occur. Chronic HDV is particularly dangerous because it advances progression to serious liver damage and liver failure much more quickly than HBV alone – 70% of people diagnosed with HDV and HBV will experience serious liver damage within 10 years without intervention, compared to 15-30% of people diagnosed with HBV alone.
So, What’s Happening in the World of Hepatitis Delta?
The past 18 months have been very important for hepatitis delta research and drug development. In July of 2020, the European Medicines Agency approved Hepcludex, the first-ever drug approved for treatment of hepatitis delta, for prescription in France, Austria, and Germany. Hepcludex works by stopping HDV from entering and infecting liver cells (and is known as an entry inhibitor). In 2021, MYR Pharma, the German company that originally developed Hepcludex, was bought by Gilead Sciences, Inc., which is based in the United States, and which has since filed a Biologics Licensing Agreement for approval of Hepcludex by the US Food and Drug Administration, which is expected later this year. At this time, there is not a timeline for when Hepcludex approval will be expanded to more countries and parts of the world. Prior to Hepcludex, the only drug available for hepatitis delta management, which was never officially approved, was called pegylated interferon alpha. This drug, still in use today, is only effective in controlling HDV in about 25% of people living with the virus and has challenging side effects that can negatively impact quality of life.
In addition to Hepcludex, two other promising drugs are in clinical trials, both developed by Eiger BioPharma in the United States. The first of these is called Lonafarnib, which is being evaluated for how well it works to target the protein assembly process, which keeps new viruses from being created (it is known as a prenylation inhibitor). Lonafarnib, in combination with another drug called Ritonavir, is currently in Phase III clinical trials (the phase in which the safety and effectiveness of a drug is compared to that of currently available treatments). These trials are fully enrolled, and data is expected by the end of 2022. Additionally, Eiger is currently enrolling phase III clinical trials for Pegylated Interferon Lambda, which works by stimulating the body’s own immune system to fight the virus. For a full list of drugs under investigation for hepatitis delta, including one from Janssen Research and Development and one from Antios Therapeutics, visit our Drug Watch page.
Are There Other Clinical Trials Happening for Hepatitis Delta?
Yes! There are clinical trials happening worldwide to test many of the drugs listed above and more. You can check out our clinical trials page here. This page includes a detailed description of each clinical trial, along with information about where it is being conducted and how to contact the principal investigator (or person leading the clinical trial). This page also includes a helpful graphic describing the clinical trial process and what it takes for a drug to move from an idea into the real world. It is important to note that not all of the trials listed here are for the purpose of testing a medication – some are observational studies to monitor what are called disease biomarkers, which are physical measures used to monitor the progress of a disease and could include tests of blood or liver function, for example. Clinical trials are currently happening in Australia, Austria, Belgium, Brazil, Bulgaria, Canada, China, France, Georgia, Germany, Greece, Israel, Italy, Japan, Mongolia, New Zealand, Pakistan, Republic of Moldova, Romania, Russian Federation, Spain, Sweden, Switzerland, Taiwan, Turkey, Ukraine, the United Kingdom, the United States, and Vietnam.
When Will HDV Drugs and Clinical Trials Be More Accessible in More Parts of the World?
This is unfortunately a difficult question to answer. Even though up to 10% of people who are living with hepatitis B are also living with hepatitis delta, there are not good systems in place to make sure that everyone who is living with HBV or who is at increased risk for HDV is tested and diagnosed, so there are not very accurate numbers about how many people in the world are living with HDV. Indeed, of the nearly 300 million people around the world who are living with hepatitis B alone, only 10% are aware of their diagnosis, so this number is undoubtedly far lower than even 10% for hepatitis delta. Without accurate information about how many people are living with the virus, it is difficult for drug and clinical trial developers to invest resources into studying or pursuing drug development or clinical trials for HDV.
Another problem is the many resources of time, money, and labor that are necessary for developing drugs, and preparing and running clinical trials. The development process for a single drug can take anywhere from 5-15 years and a much larger number of drugs fail to complete this process than succeed. Additionally, there needs to be some degree of existing infrastructure in a particular country in order to both support a clinical trial and ultimately to get a drug approved. Unfortunately, this kind of infrastructure is generally already established and easier to navigate in wealthier countries, so these are the countries in which clinical trials are generally held and in which drug approvals tend to happen first. Public health and clinical infrastructure is slowly developing and becoming more prioritized in different parts of the world and hopefully this trend will continue, but for the time being, the locations of clinical trials and approvals for important treatments point to the much larger issues of lack of access to health and healthcare in much of the world, that in turn stem from deep-seated poverty and inequity. Again, as health equity continues to be a focus of the public eye, these trends will hopefully begin to change, paving the way for greater access to healthcare for hepatitis delta, hepatitis B, and countless other health conditions.
What Is Hep Delta Connect’s Role?
This year, Hep Delta Connect will continue its work to raise the profile of hepatitis delta, both in the United States and around the world. We are committed to building awareness through partnerships with community-based organizations, healthcare providers, and governmental agencies around the world and through dissemination of educational materials and programming. We hope to foster greater engagement of those living with and affected by hepatitis delta globally, more focused advocacy efforts to bring HDV into the spotlight, and increased screening, diagnosis, and management of HDV. We keep our website and social media channels updated regularly with program news and events – make sure to follow us on Facebook, Twitter, and Instagram and check out our website frequently! You are always welcome to connect with us anytime at connect@hepdconnect.org. We look forward to an exciting year of work on HDV!
The short answer is, possibly. Although there is extensive research to support the role of hepatitis delta in accelerating the risk for progression to cirrhosis (liver scarring) compared to hepatitis B infection (1,2) only, strong data directly linking an increase in risk for hepatocellular carcinoma (HCC) is lacking. It is known that coinfection promotes continually progressing inflammation within the liver by inducing a strong immune response within the body; where it essentially attacks itself (3), but the specific role of hepatitis delta in HCC isn’t fully understood. It gets complicated because although cirrhosis is usually present in hepatitis B patients who also have HCC, but scientists have not pinpointed a specific way that the virus may impact cancer development (4). There have been some small studies that have documented a correlation between hepatitis delta and an increase in HCC, but some analysis’s have even called the extent of its involvement in HCC as ‘controversial’ (5). However, other scientific studies may suggest the contrary.
Because hepatitis delta cannot survive without hepatitis B, and doesn’t integrate into the body the same way, it may not be directly responsible for cancer development, but it has been suggested that the interactions between the two viruses may play a role (6). It has also been suggested that hepatitis delta may play a role in genetic changes, DNA damage, immune response and the activation of certain proteins within the body – similarly to hepatitis B and may amplify the overall cancer risk (7,8). One of these theories even suggests that hepatitis delta inactivates a gene responsible for tumor suppression, meaning it may actually promotes tumor development, a process that has been well-documented in HCC cases (9,10).
Regardless of the specific impact or increase in risk for HCC due to the hepatitis delta virus, hepatitis B is known to increase someone’s risk, with 50-60% of all HCC globally attributable to hepatitis B (11). People with hepatitis delta coinfection still need to be closely monitored by a liver specialist, as 70% of people with both viruses will develop cirrhosis within 5-10 years (12). Monitoring may be blood testing and a liver ultrasound to screen for HCC every 6 months. Closer monitoring may be required if cirrhosis is already present, or to monitor response to treatment (interferon).
Manesis EK, Vourli G, Dalekos G. Prevalence and clinical course of hepatitis delta infection in Greece: A 13-year prospective study. J Hepatol. 2013;59:949–956.
Coghill S, McNamara J, Woods M, Hajkowicz K. Epidemiology and clinical outcomes of hepatitis delta (D) virus infection in Queensland, Australia. Int J Infect Dis. 2018;74:123–127.
Zhang Z, Filzmayer C, Ni Y. Hepatitis D virus replication is sensed by MDA5 and induces IFN-β/λ responses in hepatocytes. J Hepatol. 2018;69:25–35.
Nault JC. Pathogenesis of hepatocellular carcinoma according to aetiology. Best Pract Res Clin Gastroenterol. 2014;28:937–947.
Puigvehí, M., Moctezuma-Velázquez, C., Villanueva, A., & Llovet, J. M. (2019). The oncogenic role of hepatitis delta virus in hepatocellular carcinoma. JHEP reports: innovation in hepatology, 1(2), 120–130.
Romeo R, Petruzziello A, Pecheur EI, et al. Hepatitis delta virus and hepatocellular carcinoma: an update. Epidemiol Infect. 2018;146(13):1612‐1618.
Majumdar A, Curley SA, Wu X. Hepatic stem cells and transforming growth factor β in hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. 2012;9:530–538.
Mendes M, Pérez-Hernandez D, Vázquez J, Coelho AV, Cunha C. Proteomic changes in HEK-293 cells induced by hepatitis delta virus replication. J Proteomics. 2013;89:24–38.
Chen M, Du D, Zheng W. Small Hepatitis Delta Antigen Selectively Binds to Target mRNA in Hepatic Cells: A Potential Mechanism by Which Hepatitis D Virus Down-Regulates Glutathione S-Transferase P1 and Induces Liver Injury and Hepatocarcinogenesis. Biochem Cell Biol. August 2018.
Villanueva A, Portela A, Sayols S. DNA methylation-based prognosis and epidrivers in hepatocellular carcinoma. 2015;61:1945–1956.
Hayashi PH, Di Bisceglie AM. The progression of hepatitis B- and C-infections to chronic liver disease and hepatocellular carcinoma: epidemiology and pathogenesis. Med Clin North Am. 2005;89(2):371‐389.
Abbas, Z., Abbas, M., Abbas, S., & Shazi, L. (2015). Hepatitis D and hepatocellular carcinoma. World journal of hepatology, 7(5), 777–786.
Eiger is currently working on two new drugs for hepatitis delta; Lonafarnib and Pegylated Interferon Lambda, which are both currently inphase 3 clinical trials. Lonafarnib is a new type of treatment that attempts to control hepatitis delta through a new method: through blocking a key enzyme that is needed for the hepatitis delta virus to replicate. Blocking this enzyme prevents a new virus from being created, which may control and even cure hepatitis delta.
Lambda is being developed as a better tolerated interferon compared to interferon alfa (IFN alfa). Interferons work by stimulating the body’s own immune system to fight the virus. Pegylated interferon alpha, which is the only current treatment for hepatitis delta, is a difficult treatment to tolerate, with many patients experiencing unpleasant side-effects. Lambda utilizes the same method of treatment as IFN alfa, in combination with a new strategy, which stimulates an immune response and targets receptors in the liver, which may reduce side effects and result in improved tolerability.
Below is Eiger Biopharmaceuticals’ response to a series of questions we posed to them.
Image courtesy of Praisaeng, at FreeDigitalPhotos.net.
1. Lambda is an immunomodulator and Lonafarnib is a prenylation inhibitor. Can you explain in laymen’s terms the mechanism for these drugs and how they work?
Eiger’s wording: Lonafarnib is a well-characterized, first-in-class, orally active inhibitor of an enzyme that is key to a vital process in the life cycle of HDV. Inhibiting this enzyme blocks the ability of HDV to assemble and package viral particles. Currently approved nucleos(t)ide treatments for HBV only suppress HBV DNA, do not affect HBsAg, and have no impact on HDV infection.
Lambda is being developed as a better tolerated interferon compared to interferon alfa (IFN alfa). Lambda is a well-characterized, first-in-class, type III interferon (IFN) that stimulates immune responses that are critical for the development of host protection during viral infections. By targeting receptors that are localized in the liver, Lambda treatment may reduce side effects and result in improved tolerability .
Can you share, in simple terms, the basic results of Eiger phase 3 studies for hepatitis delta trials? Are these drugs equally effective in HBeAg positive and negative HBV patients?
The Eiger Phase 2 LOWR program with Lonafarnib has been completed. Over 120 patients were dosed in Phase 2 dose-finding studies to identify combination regimens of lonafarnib (LNF) and ritonavir (RTV) with and without pegylated interferon-alfa (PEG IFN α), with efficacy and tolerability to enable viral load suppression of HDV RNA and ALT normalization at Week 24.
Dosing regimens of LNF 50 mg twice daily + RTV 100 mg twice daily with and without PEG IFN-a-2a 180 mcg once weekly were identified with the following reported results:
All-oral: Lonafarnib boosted with ritonavir
29% of patients achieved ≥ 2 log decline and ALT normalization
Combination: Lonafarnib boosted with ritonavir + PEG IFN-a-2a
63% of patients achieved ≥ 2 log decline and ALT normalization
These dosing arms are being further studied in the global Phase 3 D-LIVR study. Phase 2 studies have not been stratified by HBeAg status.
The D-LIVR Study, a Phase 3 pivotal trial, is on-going and evaluating the safety and efficacy of lonafarnib treatments in patients chronically infected with Hepatitis Delta Virus (HDV). Topline Week 48 data will be available in 2021.
2. How will Lambda and Lonafarnib be administered to patients?
Lonafarnib capsules are administered orally twice daily by mouth. Lonafarnib is taken in combination with ritonavir, a therapeutic booster that increases the bioavailability of lonafarnib. Ritonavir tablets are administered orally twice daily by mouth.
Pegylated interferon-lambda is administered as a self-administered subcutaneous injection once weekly.
3. Do you anticipate combination therapy will be needed and if so, which combinations do you anticipate?
No form of viral hepatitis has been cured with a single drug. Combinations of treatments with different mechanism of actions have always been required.
Lonafarnib and interferons have different mechanisms of action and have been studied as monotherapies and in combination together as treatments for HDV. While each treatment alone reduces the HDV viral load, combination studies have shown that using these treatments together leads to a synergistic effect and further reduces the HDV viral load.
Recently, the interim end of treatment results of peginterferon lambda (Lambda) and lonafarnib combination study in HDV-infected patients were presented at AASLD 2019. The LIFT study is being conducted within the National Institutes of Health (NIH) at the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). LIFT is a Phase 2a open-label study of 26 adult patients with chronic HDV treated with Lambda 180 mcg once weekly in combination with Lonafarnib 50 mg twice daily boosted with ritonavir 100 mg twice daily for 24 weeks. Primary efficacy endpoint is > 2 log HDV RNA decline at end of treatment. At the time of analysis, 19 of 26 patients had reached Week 24. Median HDV RNA decline was 3.4 log IU/mL (IQR: 2.9-4.5, p<0.0001) with 53% (10 of 19) patients achieving below the limit of quantification and 37% (7 of 19) patients achieving undetectable HDV RNA at Week 24. 18 of 19 patients (95%) achieved primary endpoint of > 2 log decline during 24 weeks of therapy. We believe these data are the most encouraging yet in pursuit of HDV cure.
4. What kind of side effects can patients expect with Lambda and Lonafarnib, with or without combination therapy?
The most common side effects of lonafarnib include diarrhea, nausea, fatigue, decreased appetite, vomiting, abdominal pain, and decreased weight. Antacid, antiemetic, and antidiarrheal medications may be used prophylactically to treat these gastrointestinal side effects.
The most common side effects of pegylated interferon-lambda (Lambda) are the expected side effects of interferons. However, these side effects have been demonstrated to be much milder and less severe than what has been previously been shown with pegylated interferon-alfa (alfa). These include musculoskeletal (myalgia, arthralgia, and back pain), flu-like symptoms (chills, pyrexia, and pain) and elevated alanine aminotransferase (ALT) levels.
A combination of these side effects is expected with combination therapy.
5. Are Lambda and Lonafarnib safe for use in people with cirrhosis?
Currently, the safety and efficacy of lonafarnib and pegylated interferon-lambda are being investigated in persons chronically infected with HDV. The clinical trials require study participants meet certain eligibility criteria to be included in these studies. These eligibility criteria may or may not reflect the type of patient who will use these therapies after they receive FDA approval.
Phase 2 and Phase 3 studies both include patients with well-compensated cirrhosis.
6. With a clearance of HDV, would you also anticipate a loss of surface antigen – functional cure for chronic HBV as well? If so, in what percentage of HBeAg and HBeAb patients?
HDV is always found as a co-infection with HBV because HDV requires just a small amount of HBV surface antigen (HBsAg) to complete HDV viron replication. However, an HDV / HBV coinfection leads to much more severe chronic viral hepatitis compared to HBV monoinfection alone. Therefore, it is important to treat HDV, even if HBV is not cured. It is possible to clear HDV RNA without loss of HBsAg.
7. Lambda and Lonafarnib are currently in phase 3 trials for delta. Are you able to provide an approximate timeline for when it will be approved for use in U.S. and Europe?
Eiger BioPharmaceuticals is committed to developing safe and effective therapies for HDV and providing patients with a pathway to gain access to approved therapies as quickly as possible.
The D-LIVR Study is a global study that is evaluating the safety and efficacy of lonafarnib treatment in patients chronically infected with HDV. The D-LIVR Study is recruiting subjects in up to 20 countries in over 100 study sites. The D-LIVR study includes 48 weeks of treatment with two different lonafarnib-based treatment regimens, followed by 24 weeks of follow-up. Primary endpoint is ≥ 2 log decline and ALT normalization at Week 48. Topline data from the Phase 3 D-LIVR study will be available in 2021. For more information about study locations and eligibility, please visit www.clinicaltrials.gov (NCT03719313).
End of Phase 2 meeting with FDA to discuss Phase 3 development with Lambda monotherapy is planned for Q1 2020.
For people who have been diagnosed with chronic hepatitis B and delta coinfection, a low or undetectable hepatitis B viral load does not usually indicate that they’ve cleared both infections. This is because, in cases of coinfection, hepatitis delta usually becomes the dominant virus, and suppresses hepatitis B, slowing or even stopping its replication entirely. If someone is still positive for the hepatitis B surface antigen (HBsAg), the hepatitis delta virus can still replicate (often with copies in the millions) and cause potential liver damage 1. For this reason, the test to measure hepatitis delta activity, the HDV RNA test, is important in disease monitoring and management 2,3. Available since 2013, the HDV RNA test can be acquired internationally through the Centers for Disease Control and Prevention (CDC), and from several labs in the US.
For those suspected of having acute hepatitis B and delta coinfection, HBsAg testing should follow 6 months after initial diagnosis. If HBsAg is negative (non-reactive), both infections are likely to have cleared.It’s important to remember that people who contract hepatitis B and delta during one exposure are likely to clear both viruses. If HBsAg is positive (reactive) after 6 months, both infections are likely chronic (life-long).Those who are known to have a chronic hepatitis B infectionand then become infected with hepatitis delta later on, they are likely to develop chronic coinfections.
Following diagnosis with hepatitis B, with or without delta coinfection, it is important to have close, household contacts and sexual partners screened, and to follow simple prevention measures and practice safe sex using condoms.
Huang, C. R., & Lo, S. J. (2014). Hepatitis D virus infection, replication and cross-talk with the hepatitisB virus. World journal of gastroenterology, 20(40), 14589–14597.
YurdaydınC, Tabak F, Idilman R; Viral Hepatitis Guidelines Study Group. Diagnosis, management and treatment of hepatitis delta virus infection: Turkey 2017 Clinical Practice Guidelines. Turk J Gastroenterol 2017; 28(Suppl 2); S84-S89. Available at: https://www.turkjgastroenterol.org/sayilar/304/buyuk/S84-S89.pdf
Tseng, C. H., & Lai, M. M. Hepatitis delta virus RNA replication.Viruses, 1(3), 818–831.
By Sierra Pellechio, BS, CHES, Hepatitis Delta Connect Program Manager
Historically, testing for hepatitis delta has been difficult to access and often not commercially available. With the rise in awareness about hepatitis B and delta coinfection, more tests are beginning to be offered by multiple labs for clinicians in the United States looking to test their patients. Because hepatitis delta can only infect people who also have hepatitis B, the Hepatitis B Foundation’s medical director and leading hepatologist Dr. Robert Gish recommends testing all hepatitis B patients for hepatitis delta. “Screening all hepatitis B patients will allow a better understanding of hepatitis delta prevalence and its impact on outcomes and will identify patients who can be offered treatment within or outside clinical trials.”
The first step in diagnosing an infection is the HDV antibody total (anti-HDV) test. Patients who have recovered from or are currently infected will be positive for the anti-HDV and will present high titers in later stages of acute infection and persist in cases of chronic infection. If the HDV antibody total test is positive, it should be followed by the HDV RNA (PCR) test to confirm an active infection. If this test is negative, a current infection is unlikely.
Testing hepatitis B patients for hepatitis delta is important because when people with hepatitis B are exposed to the hepatitis delta virus, 90% will develop a chronic infection1. Coinfection will alter treatment and management plans, because antivirals effective on hepatitis B do not control hepatitis delta2. While the standard treatment of interferon is less than 30% effective in controlling coinfection, there are new drugs in development. With two of these drugs set to enter phase 3 clinical trials in 2019, it is more important than ever to identify coinfected patients and connect patients into clinical trials.
Until recently, only the anti-HDV test was widely available in the United States. In February 2019, Quest Diagnostics began offering HDV RNA testing, making it easier for patients and their physicians to access this more detailed level of testing. A complete list of labs offering testing is below.
Disclaimer:This may not be a comprehensive list of all available labs offering testing.
Please note, if you are a patient in the U.S. and wish to be tested for hepatitis delta, these tests must be ordered through a clinician.
It is very important for coinfected patients to be managed by a liver specialist who is familiar with managing coinfected patients. For assistance in locating a specialist near you, please visit our Physician Directory page. For additional questions, please visit www.hepdconnect.org, email connect@hepdconnect.org, or call our hotline at 215-489-4900.
References:
Hooks, B., Billings, J., & Herrera, J. (2009). Hepatitis D Virus. Practical Gastroenterology.
2. Farci, P., & Anna Niro, G. (2018). Current and Future Management of Chronic Hepatitis D. Gastroenterology & hepatology, 14(6), 342-35
By Sierra Pellechio, Hepatitis Delta Connect Coordinator
Hepatitis delta is an aggressive form of hepatitis that can only exist alongside hepatitis B. This means that all hepatitis B patients are at risk for hepatitis delta, but so are people who have not received the hepatitis B vaccination series.
If contracted, 70-90% of people with chronic hepatitis B will go on to also develop a chronic hepatitis delta infection – called a “superinfection”. Approximately 70% of these cases will progress to cirrhosis (liver scarring), compared to 15-30% of those infected only with the hepatitis B virus.
Due to the likelihood of liver complications, hepatitis B patients should be aware of potential exposures to hepatitis delta. The virus is spread the same way as hepatitis B, through direct blood-to-blood contact and unprotected sex with an infected person. It is important to be aware that blood contact could also occur by exposure to unsafe blood transfusions, unsterile medical or dental equipment, and the sharing of razors or toothbrushes with an infected person due to the possibility of infected blood entering the body.
People who are not infected with hepatitis B may be at risk for “coinfection”, when someone contracts hepatitis B and delta simultaneously during one exposure. In these cases, greater than 90% of adults will clear both infections and develop protective antibodies. While a co-infection generally resolves spontaneously after about 6 months, it can sometimes result in a life-threatening or fatal liver failure.
The good news is that the hepatitis B vaccine series can prevent both viruses in people who are not already infected. Once completed, the vaccine can provide a lifetime of protection!
Although there are highly effective treatments available to manage hepatitis B, there are few available treatments for hepatitis D, and none are U.S. Food and Drug Administration (FDA) approved. Hepatitis D is the most severe form of viral hepatitis, and coinfection can accelerate liver damage and cause cirrhosis or liver cancer in as little as 5 years for some patients. Currently there is no approved drug for acute or chronic hepatitis B/D coinfection, but in trials pegylated interferon alpha has shown to be somewhat effective. By stimulating the body’s immune system, around 25-30% of patients are able to suppress their hepatitis D viral load with weekly injections over 48 weeks. Emerging research is showing higher rates of effectiveness with prolonged interferon treatment beyond one year, but it can be difficult for patients to continue due to the physical and mental toll of interferon on the body. Antiviral medications that are proven effective against hepatitis B are sometimes prescribed along with interferon therapy for patients with a high hepatitis B viral load, but these have no effect on hepatitis D. It is urgent that more treatment options be developed for the millions of hepatitis B/D patients that are eagerly awaiting them.
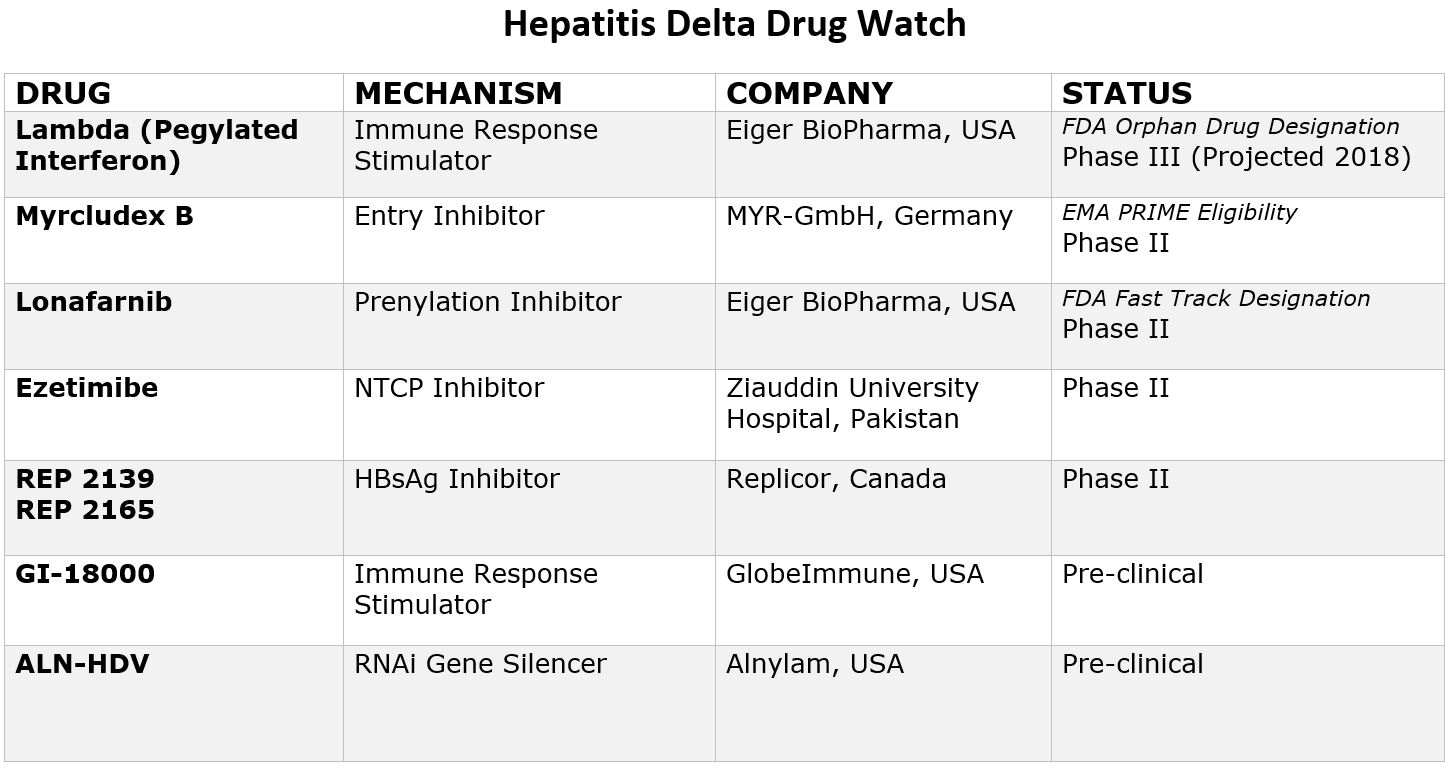
The good news is that with renewed scientific interest, research and funding, eight new drugs are currently in development that offer hope for more treatment options in the coming years. Two drugs have even been granted special designations by the FDA and one by European Medicines Agency (EMA), paving the way for increased resources and funding for development. Due to recent advancements, the future looks hopeful, and within a few years it is likely there will be more treatment options available. Below is a chart that provides more information on these new drugs and their current clinical trial status.
Pegylated Interferon Lambda
Pegylated-interferon-lambda (PEG-IFN-λ) is a well-characterized, late-stage, first in class, type III interferon that stimulates cell-mediated immune responses that are critical for the development of host protection during viral infections. This drug has now been granted “Orphan Drug Designation” by the FDA, fast-tracking the development process.
Myrcludex B
This drug is an “entry inhibitor” that prevents the virus from entering into hepatocytes (liver cells) and has shown activity against the hepatitis B virus. It may also stop the development of a hepatitis D infection. A recent study showed promise for Myrcludex B when combined with PEG-INF in reducing hepatitis D viral levels. It has been granted PRIME Eligibility by the European Medicines Agency, a status that promotes support in development of drugs that serve an unmet medical need.
Ezetimibe
Currently used to lower cholesterol in the blood, Ezetimibe is being studied for effectiveness against hepatitis D. Ezetimibe possesses pharmacophore features to stop NTCP, the receptor required for hepatitis B and hepatitis D hepatocyte entry.
Lonafarnib
This drug works by targeting the protein assembly process, preventing the production of new virus particles. In a current clinical trial, Lonafarnib combined with Ritonavir has shown promise in reducing hepatitis D viral levels, and the FDA has granted it fast-track status since this class of drugs have been developed for the treatment of cancers and have been shown to be safe.
Rep 2139
This compound is known as a “Nucleic acid-based Amphipathic Polymer” (NAP) which prevents the release of hepatitis B surface antigen (HBsAg) from infected liver cells and is being evaluated for hepatitis D virus in combination with pegylated interferon (PEG IFN).
GI-18000
GI-18000 Tarmogen is being studied for its effectiveness in causing a T cell immune response against cells infected with Hepatitis D and thereby improving outcomes. The strategy is to identify molecular targets that distinguish diseased cells from normal cells and activate the immune system to selectively target and eliminate only the diseased cells.
ALN-HDV
This approach is being used for both the hepatitis B and hepatitis D virus to “silence” the viral RNA with compounds that interfere with and cause the destruction of the viral genome (e.g. stop replication of the virus).
As clinical trials progress, sites may open across the world that are enrolling hepatitis D patients. Keep checking here for an up-to-date list of all current clinical trials.
Click here for more information about the phases of the clinical trial process.
By Sierra Pellechio, Hepatitis Delta Connect Coordinator
Hepatitis delta, or hepatitis D, is an aggressive form of hepatitis that can only infect someone who is also infected with hepatitis B.
People can become infected with hepatitis B and hepatitis D from the same exposure, or people who are already infected with hepatitis B can later be infected with hepatitis D. Coinfection can promote more rapid progression to cirrhosis and liver cancer than being infected with hepatitis B alone and will require an altered treatment and management plan. Being aware could save your life!
Hepatitis D can be spread similarly to hepatitis B, through exposure to blood or bodily fluids of an infected person. People with hepatitis B are likely to develop a chronic hepatitis delta coinfection if they are exposed to the virus, making it important for you and your doctor to be aware of the signs of a coinfection.
Cues to suspect a coinfection:
You have chronic hepatitis B but are not responding to antiviral treatment, or you have signs of liver damage even though your viral load is low (HBV DNA below 2,000 IU/mL)
Note: Fatty liver disease (caused by obesity) and liver damage from alcohol or environmental toxins should be ruled out as causes of liver damage before testing for hepatitis D.
It is also important for hepatitis B patients who originate from Sub-Saharan Africa, China, Russia, the Middle East, Mongolia, Romania, Georgia, Turkey, Pakistan and the Amazonian River Basin to be tested for hepatitis D, where it is more common. Most of the time, patients do not have any signs or symptoms to let them know they are coinfected, so a simple blood test is the only way to know for sure! Talk to your liver specialist about testing at your next appointment.
Hepatitis Delta Connect is a dedicated program of the Hepatitis B Foundation aimed to provide information and support for those affected by hepatitis D. Please visit our website, www.hepdconnect.org for more information and follow us on Facebook, Twitter and Instagram to stay up to date on the latest hepatitis D news! If you are a patient or provider and have questions or concerns, please email us at connect@hepdconnect.org.
Check out our previous posts about hepatitis D here, here, and here.
Are you or someone you know at risk for hepatitis B? You might be more at risk than you think, and since hepatitis B is vaccine preventable, it makes sense to get tested and vaccinated for HBV. Hepatitis Bis the number one cause of liver cancer worldwide. The survival statistics for liver cancer are particularly grim, with a relative 16,6% 5-year survival rate. The hepatitis B vaccine also protects against hepatitis delta, the most severe form of viral hepatitis.
It is important to note that everyone is susceptible to hepatitis B. It does not discriminate. It infects, babies, children, teens, adults and seniors. It has no racial or religious bias, though it is certainly more prevalent among certain ethnic groups –mainly because it is endemic to the homelands of these communities. For example, if you look at the prevalence map for hepatitis B, you will see that in most of the world, hepatitis B is at an intermediate, (2-7%) or high HBsAg prevalence (>8%) level. Looking at the numbers, 2 billion people in the world, that’s 1 out of 3 people, have been infected with HBV and 257 million are chronically infected. That represents three-quarters of our world. Even if you aren’t living in these parts of the world, you may be traveling to some of these areas for work or pleasure, or perhaps your parents and other family members were born in HBV endemic areas. Since there are often no symptoms for HBV, and screening and vaccination may be lacking in some populations, HBV is transmitted from one generation to the next, with many completely unaware of their HBV status – until it’s too late.
Health care providers and emergency responders due to the nature of their work and potential for exposure.
Sexually active heterosexuals (more than 1 partner in the past six months)
Men who have sex with men (MSM)
Individuals diagnosed with a sexually transmitted disease (STD)
Illicit drug users (injecting, inhaling, snorting, pill popping)
Sex contacts or close household members of an infected person (remember, you may not know who is or is not infected)
Children adopted from countries where hepatitis B is common (Asia, Africa, South America, Pacific Islands, Eastern Europe, and the Middle East) and their adopted families
Individuals emigrating from countries where hepatitis B is common (see above)
Individuals born to parents who have emigrated from countries where hepatitis B is common (see above)
ALL pregnant women – because infants are so vulnerable to HBV (90% of infected infants will remain chronically infected, and HBV is very effectively transmitted from infected mother to baby.)
Recipients of a blood transfusion before 1992
Recipients of unscreened blood and blood products – sadly an issue in many parts of the world.
Recipients of medical or dental services where strict infection control practices are not followed – sadly another issue in parts of the world.
Kidney dialysis patients and those in early renal failure
Inmates of a correctional facility
Staff and clients of institutions for the developmentally disabled
Individuals with tattoos and body piercings performed in a parlor that does not strictly adhere to infection control practices – it may be up to you to ensure proper infection control practices are followed.
People living with diabetes are at risk if diabetes-care equipment such as syringes or insulin pens are inadvertently shared.
The good news is that hepatitis B is a vaccine preventable disease. There is a safe and effective, 3-shot HBV vaccine series that can protect you and your loved ones from possible infection with HBV. The earlier you are vaccinated, the better. In the US, a birth dose of the vaccine is recommended for all infants, since these little ones are most vulnerable to hepatitis. (90% of infected infants will live with HBV for life). HBV vaccination doesn’t give you a free-pass from other infectious diseases such as HCV or HIV, both without vaccines, so strict infection control practices should still be followed. However, HBV is a tenacious virus that survives outside the body for a week and is 50-100 times more infectious than HIV 3-5 times more infectious than HCV. Plus the HBV vaccine is actually an anti-cancer vaccine, so why not get vaccinated?
Hepatitis B isn’t casually transmitted, but in the right scenario, it is effectively transmitted. You may think that situation may never come about for you, or for your loved ones –especially your little ones who are so vulnerable to HBV. Some people travel to exotic lands with unsafe blood supplies and poor infection control practices, and sometimes they get sick, or require emergency dental or medical services, so they may be put at risk. Most people have had a lapse in judgment – sometimes it’s a one-time thing, sometimes it lasts for years, but the net-net is that it’s unusual to find someone who has not engaged in some sort of high-risk activity, whether intentionally or unintentionally. If you are properly vaccinated to protect against hepatitis B, you can cross that concern off your list.
B sure. Get screened. if you do not have HBV, get vaccinated and be hepatitis B free. If you discover you have HBV, talk to your doctor and have him refer you to a liver specialist who can better evaluate your hepatitis B status and your liver health.






 By Sierra Pellechio, Hepatitis Delta Connect Coordinator
By Sierra Pellechio, Hepatitis Delta Connect Coordinator