Hepatitis B is a liver infection which is caused by the hepatitis B Virus (HBV). Hepatitis B is transmitted from person to person through blood, semen, or other bodily fluids. You can learn more about the ways hepatitis B is spread here. People who inject drugs (PWID) are at high risk for contracting the virus due to the sharing of needles and low awareness and education about hepatitis B.
HBV Prevalence among PWID Communities
People who inject drugs (PWID) are at high risk for hepatitis B virus infection due to various factors, including sharing injection equipment and lack of awareness about hepatitis B transmission. Using unclean needles to inject drugs can result in the exchange of blood. This increases a person’s risk of being exposed to the virus. Hepatitis B prevalence among PWID is much higher than in the general population. Chronic HBV infection has been identified in 3.5% to 20.0% of PWID in a variety of settings, and 22.6% of PWID have evidence of past infection (Haber & Schillie, 2021). Drug injection is the most common risk for persons ages 18-40 years old with hepatitis B virus.
Barriers to Care for PWID Communities
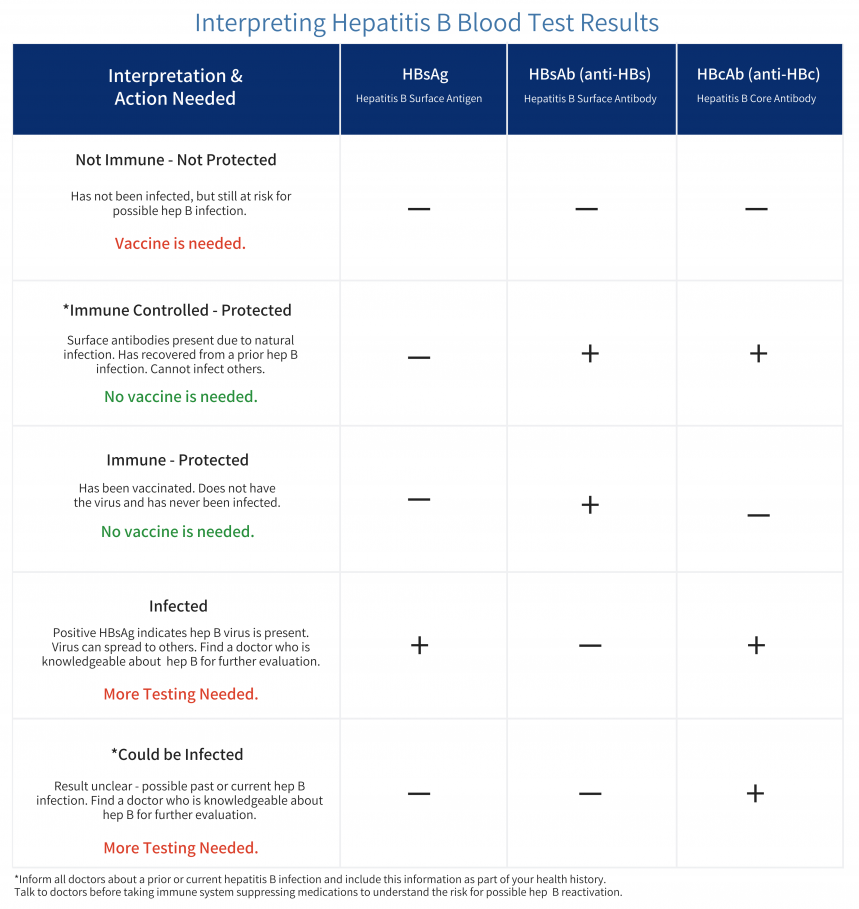
Access to treatment can be a significant barrier for PWID, who may face stigma and discrimination in healthcare settings. To find out if someone has hepatitis B it is recommended that a triple panel hepatitis B test be run (which includes HBsAg, HBcAb and HBsAb). These tests will help identify people with hepatitis B, a previous exposure to hepatitis B and those who have protection against hepatitis B infection (through vaccination). For those with hepatitis B, treatment options for hepatitis B consist of antiviral medications that can help to control the virus and reduce the risk of serious liver damage, cirrhosis, and liver cancer. Treatment is taken daily for life generally. PWID lack access to these treatments due to the stigma attached with substance use and addiction. Some of these stigmas include being associated with dangerous, unpredictable, and lacking self-control (NIH, 2019). In a recent study, 88% of individuals from PWID have experienced some type of stigma from the healthcare system (NIH, 2019). Some of these stigmas included being poorly treated in healthcare facilities while interacting with nurses, security guards, and other medical providers. Due to these biases, people often refuse to seek health care services to avoid mistreatment. Stigma is the top barrier for PWID communities worldwide (Biancarelli et al, 2019). Even though the cost of treatment may be a barrier for some people, there are resources to find affordable options. Learn more about accessing medication here.
Prevention Strategies
One effective prevention strategy to combat the spread of hepatitis B among PWID is to use clean injection equipment, like needles, works, and syringes. This will reduce the likelihood of transmission. New services have been introduced in cities like Philadelphia to decrease the rate of sharing needles. Prevention Point Philadelphia for example is a nonprofit public health organization that works to provide comprehensive harm reduction services to Philadelphia and surrounding areas. The syringe service program specifically allows used syringes to be exchanged for clean ones. With these services, the need to share needles can decline, which then can help decrease the risk of hepatitis B and other infectious diseases being spread in the community. Needle and syringe programs also provide other social and health services, such as counseling, hepatitis testing, and referral to drug treatment for example.
Another way to prevent hepatitis B in PWID is through education and outreach efforts to help raise awareness about the risks of transmission and how to reduce those risks. This will also encourage safer injection practices to reduce the risk of transmission through blood contact. Other recommendations for prevention of hepatitis B among people who inject drugs is to offer vaccinations for PWID communities. The hepatitis B vaccine is safe and effective and recommended for all adults in the US between the ages of 18-59 and above 59 with risk factors. Testing is another great way to help the community- to identify infection and encourage prevention through vaccination ultimately preventing liver cancer in the long run. Offering people who inject drugs incentives to increase uptake and complete the vaccination schedule is also a way to prevent hepatitis B in PWID (WHO, 2023). The United States has set a goal to decrease the number of cases of hepatitis B in the PWID community. The National Progress Report goal is to reduce the rate of new hepatitis B virus infections among people who inject drugs by more than 25% by 2025 (CDC, 2020).
To learn more about the resources provided by Prevention Point, click here.
References:
World Health Organization. (2022, June 24). Hepatitis B. World Health Organization. Retrieved March 15, 2023, from https://www.who.int/news-room/fact-sheets/detail/hepatitis-b
World Health Organization. (2015, March). Guidelines for the prevention, care and treatment of persons with chronic hepatitis B infection. World Health Organization. Retrieved March 15, 2023, from https://www.who.int/publications/i/item/9789241549059
Centers for Disease Control and Prevention. (2020, August 11). NP report 2025 goal: Reduced HBV rate among PWID. Centers for Disease Control and Prevention. Retrieved March 15, 2023, from https://www.cdc.gov/hepatitis/policy/NPR/2020/NationalProgressReport-HepB-ReduceInfectionsPWID.htm
Biancarelli DL, Biello KB, Childs E, Drainoni M, Salhaney P, Edeza A, Mimiaga MJ, Saitz R, Bazzi AR. Strategies used by people who inject drugs to avoid stigma in healthcare settings. Drug Alcohol Depend. 2019 May 1;198:80-86. doi: 10.1016/j.drugalcdep.2019.01.037. Epub 2019 Mar 8. PMID: 30884432; PMCID: PMC6521691.
Haber, P., & Schillie, S. (2021, August 18). Pinkbook: Hepatitis B. Centers for Disease Control and Prevention. Retrieved March 24, 2023, from https://www.cdc.gov/vaccines/pubs/pinkbook/hepb.html
Centers for Disease Control and Prevention. (2023, March 17). QuickStats: Age-adjusted drug overdose death rates, by state – National Vital Statistics System, United States, 2021. Centers for Disease Control and Prevention. Retrieved March 19, 2023, from https://www.cdc.gov/mmwr/volumes/72/wr/mm7211a7.htm?s_cid=mm7211a7_e&ACSTrackingID=USCDC_921-DM101471&ACSTrackingLabel=This+Week+in+MMWR+-+Vol.+72%2C+March+17%2C+2023&deliveryName=USCDC_921-DM101471
Board of Health, Department of Public Health. (2022, October 26). Health Department releases data on 2021 overdose deaths in Philadelphia: Department of Public Health. City of Philadelphia. Retrieved March 20, 2023, from https://www.phila.gov/2022-10-26-health-department-releases-data-on-2021-overdose-deaths-in-philadelphia/
 Yufei Zhao is 45 years old and lives with his family in Philadelphia, Pa. Yufei discovered that he had hepatitis B when he attended a community health fair with his family. Even though he was instructed to talk about his diagnosis with a doctor and learn more about possible treatment options, Yufei decided to do nothing as he did not feel sick. While he has health insurance through his employer, he never utilizes any health care services. He often skips annual wellness visits as he says he “never gets sick.”
Yufei Zhao is 45 years old and lives with his family in Philadelphia, Pa. Yufei discovered that he had hepatitis B when he attended a community health fair with his family. Even though he was instructed to talk about his diagnosis with a doctor and learn more about possible treatment options, Yufei decided to do nothing as he did not feel sick. While he has health insurance through his employer, he never utilizes any health care services. He often skips annual wellness visits as he says he “never gets sick.”  A few weeks ago, Yufei’s family noticed that he has been skipping meals frequently saying he’s full or not hungry. At his daughter’s urging, he decided to go for a visit. After conducting some more tests, his doctor explained that the chronic infection with the hepatitis B virus had progressed substantially, and he had developed cirrhosis. After an MRI diagnosis, it was revealed that Yufei had liver cancer
A few weeks ago, Yufei’s family noticed that he has been skipping meals frequently saying he’s full or not hungry. At his daughter’s urging, he decided to go for a visit. After conducting some more tests, his doctor explained that the chronic infection with the hepatitis B virus had progressed substantially, and he had developed cirrhosis. After an MRI diagnosis, it was revealed that Yufei had liver cancer The Hepatologist (liver doctor) explained to Yufei that the liver is an important organ and acts as a cleaning system for the body. It removes toxic waste, purifies blood, and helps to digest food properly. When the virus entered the liver, it made many copies of itself and started attacking healthy liver cells. This led to inflammation and weakened the ability of the liver to carry out its most essential tasks. Because he was never monitored for hepatitis B, the virus allowed tumors to grow in the liver which caused the cancer. When the tumors grow in size or number, it eventually spreads to other parts of the body and disrupts other vital processes as well.
The Hepatologist (liver doctor) explained to Yufei that the liver is an important organ and acts as a cleaning system for the body. It removes toxic waste, purifies blood, and helps to digest food properly. When the virus entered the liver, it made many copies of itself and started attacking healthy liver cells. This led to inflammation and weakened the ability of the liver to carry out its most essential tasks. Because he was never monitored for hepatitis B, the virus allowed tumors to grow in the liver which caused the cancer. When the tumors grow in size or number, it eventually spreads to other parts of the body and disrupts other vital processes as well. The doctor mentioned that liver cancer is often called the silent disease because symptoms may not always be present. Even with a hepatitis B, a person could look or feel okay but that does not mean the virus isn’t active and causing damage. When the symptoms do show up, it might be too late to prevent liver cancer. After discussing his options with the doctor, Yufei learned that the best treatment for him was to get a liver transplant.
The doctor mentioned that liver cancer is often called the silent disease because symptoms may not always be present. Even with a hepatitis B, a person could look or feel okay but that does not mean the virus isn’t active and causing damage. When the symptoms do show up, it might be too late to prevent liver cancer. After discussing his options with the doctor, Yufei learned that the best treatment for him was to get a liver transplant.