

Approximately 5-10% of people do not develop protective antibodies following the completion of the hepatitis B vaccine series. This is confirmed with a blood test called an anti-HBs titer test which is given 4 weeks following the completion of the series. If the test shows the titer is less then 10 mIU/mL the general recommendation is to complete the series again using a different brand of vaccine (e.g. if you received Engerix B, the first time, switch to Recombivax the 2nd time or vice-versa). A person is considered to be a “non-responder” if they have completed 2 full vaccination series’ without producing adequate protective antibodies.
Another vaccine option is the new two-dose hepatitis B vaccine, HEPLISAV-BTM. The new vaccine is expected to increase immunization rates for adults in the United States and is administered over a one-month period. The vaccine provides greater seroprotection, which can mean a greater antibody response especially in adults who may be older, obese or live with type 2 diabetes making it an effective vaccine option.
It is also possible that a person who does not respond to the vaccine may already be infected with hepatitis B. Therefore, testing for the presence of the hepatitis B virus (hepatitis B surface antigen or HBsAg) is recommended before diagnosing a person as a “vaccine non-responder.”
CDC Recommendations for Hepatitis B Vaccine Non-Responders
- Persons who do not respond to the primary hepatitis B vaccine series (i.e., anti-HBs <10 mIU/mL) should complete a second 3-dose vaccine series or be evaluated to determine if they are HBsAg-positive. Persons who do not respond to an initial 3-dose vaccine series have a 30%–50% chance of responding to a second 3-dose series.
- Revaccinated persons should be retested at the completion of the second vaccine series, 1-2 months following the last shot of the series.
- Persons exposed to HBsAg-positive blood or body fluids who are known not to have responded to a primary vaccine series should receive a single dose of hepatitis B immunoglobulin (HBIG) and restart the hepatitis B vaccine series with the first dose of the hepatitis B vaccine as soon as possible after exposure. Alternatively, they should receive two doses of HBIG, one dose as soon as possible after exposure, and the second dose 1 month later.
- The option of administering one dose of HBIG and restarting the vaccine series is preferred for non-responders who did not complete a second 3-dose vaccine series.
- For persons who previously completed a second vaccine series but failed to respond, two doses of HBIG are preferred.
Hepatitis B vaccine “non-responders” who test negative for hepatitis B infection are at risk for being infected and should be counseled regarding how to prevent a hepatitis B infection and to seek immediate medical care to receive a dose of hepatitis B immunoglobulin (HBIG) if they have been exposed to potentially infected blood.
“Non-responders” who test negative for hepatitis B infection as well as friends and family members should practice ways to prevent the spread of hepatitis B, including washing hands, using condoms during sex, avoid direct contact with blood and bodily fluids, and more.
Hepatitis B vaccine “non-responders” to vaccination who test positive for hepatitis B infection should be counseled regarding how to prevent transmitting the hepatitis B virus to others and the need for regular medical care and monitoring for their chronic infection.
In the case of possible exposures to HBV infected blood or body fluids, it is recommended that non-responders receive 2 doses of hepatitis B immunoglobulin (HBIG) – the first dose should be given within 24 hours of the exposure, and the second dose should be given 1 month later. The CDC has recommendations online for what to do in case a susceptible person is possibly exposed to the hepatitis B virus.
Check out our previous post on the topic here.
References:
CDC Guidance for Evaluating Health-Care Personnel for Hepatitis B Virus Protection and for Administering Postexposure Management. Retrieved from: https://www.cdc.gov/mmwr/preview/mmwrhtml/rr6210a1.htm
HEPLISAV-B. Retrieved from: https://heplisavb.com/

 March 27th is
March 27th is  Around the world, the most common mode of hepatitis B transmission is from mother to child. Unfortunately, pregnant mothers who have hepatitis B can transmit the virus to their newborn during the delivery process. 90% of these HBV infected babies will progress to chronic infection putting them at increased risk of serious liver disease or liver cancer later in life.
Around the world, the most common mode of hepatitis B transmission is from mother to child. Unfortunately, pregnant mothers who have hepatitis B can transmit the virus to their newborn during the delivery process. 90% of these HBV infected babies will progress to chronic infection putting them at increased risk of serious liver disease or liver cancer later in life.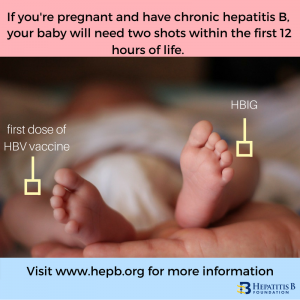 The
The  Around the world, millions of people with chronic hepatitis B face wrenching discrimination that limits their dreams, education, careers, income and personal relationships.
Around the world, millions of people with chronic hepatitis B face wrenching discrimination that limits their dreams, education, careers, income and personal relationships.

 Have you been thinking about adoption for a long time or have been inspired by NBC’s show, This is Us, to adopt? Adoption is exciting! However, it can be nerve wracking and feel overwhelming. We at the Hepatitis B Foundation can help with one aspect of the adoption process – making sure you have accurate information about hepatitis B.
Have you been thinking about adoption for a long time or have been inspired by NBC’s show, This is Us, to adopt? Adoption is exciting! However, it can be nerve wracking and feel overwhelming. We at the Hepatitis B Foundation can help with one aspect of the adoption process – making sure you have accurate information about hepatitis B.