Happy Lunar New Year! This year is the Year of the Tiger. The Tiger is a symbol of strength and bravery. Let’s go into this Lunar New Year with strength and bravery. When we are first diagnosed with a health condition, it just does not affect us physically, but mentally and emotionally. Many of us experience fear, anger, sadness, depression, anxiety, and powerlessness. Being diagnosed with hepatitis B can be scary – you might not feel strong or brave, and that is okay! The great news is that you can live a long and healthy life with hepatitis B.
Anger is a natural emotion we might experience when we are first diagnosis with hepatitis B. You might ask yourself: how did this happen to me, and why did this happen to me? It is normal to feel this way, you just got unexpected news. You might feel anger or hostility to our parents or lovers who also did not know they had the virus and passed it on to us. Talk about your anger and frustrations with a close friend or a professional counselor. You can also use healthy coping mechanisms like exercising or meditation. After we process our anger, it is important to inform close contacts (sexual partners, people who live in the same household) of your hepatitis B status so they can get tested, and vaccinated if necessary.
Sometimes this anger can turn into sadness. Prolonged sadness is also a natural emotion you can experience when you find out you are newly with hepatitis B. If you feel this prolonged sadness, anxiety, or fear, or sleeplessness, it is time to talk to someone who can help. Our fears and anxieties can sometimes overwhelm us because we do not know what is going to happen next, but know you have a support system. If you need support, you can join Hep B Community. This online group is a global peer-led, volunteer-driven forum to support to those living with and affected by hepatitis B. They are dedicated to connecting people affected by hepatitis B with each other and with verified experts in the field, who provide trustworthy and accurate advice.
Your doctor may recommend treatment after interpreting your hepatitis B test results. The great news is that hepatitis B can be successfully managed through treatment and living a healthy lifestyle by exercising and eating foods that nourish our body. When you manage your hepatitis B, you can live your life to the fullest. As you process our initial reactions and emotions, know that you are strong and brave. Living with hepatitis B is part of us, but it does not define us.
Every year on July 28th, we celebrate World Hepatitis Day in honor of Dr. Baruch Blumberg’s birthday. Dr. Blumberg discovered the hepatitis B virus in 1967 and subsequently developed the hepatitis B vaccine two years later in 1969. We commemorate World Hepatitis Day by raising awareness about viral hepatitis. With almost 300 million individuals living with hepatitis B worldwide, it is so important to bring awareness to this preventable and treatable disease. This year’s World Hepatitis Day theme is “Hepatitis Can’t Wait”. The theme focuses on the fact that people with viral hepatitis need action now – to make sure they have access to testing and treatment to save their lives.
Get Involved
Here are some ways you can get involved with World Hepatitis Day!
Share on Social Media
You can get involved with the Hepatitis Can’t Wait campaign by doing 1-minute actions, 10-minute actions, or longer actions! Your actions can be as simple as sharing a post on social media or more involved like getting in contact with your policymaker to encourage viral hepatitis prioritization
Discrimination Registry
If you are experiencing discrimination due to your hepatitis B status, consider adding your story to our discrimination registry. We are working to document discrimination related to hepatitis B. Discrimination is definedas the unjust, unfair or prejudicial treatment of a person on the grounds of their hepatitis B status. In other words, being treated differently because of one’s hepatitis B infection. For someone with hepatitis B, this can mean exclusion, denying benefits, denied employment, education, training, goods or services, or having significant burdens imposed on an individual due to their infection status.
Become an Advocate
Become a Hep B Advocate! Sign up below to receive the latest news and updates about hep B policy issues, learn about upcoming advocacy events, and be notified of opportunities to take action and show your support for our policy initiatives. We’ll provide resources, information, and tools to help you:
Communicate effectively with your elected officials
Educate and engage your community on hep B policy issues
Recruit and organize other hep B advocates and champions in your community
Promote and participate in ongoing national, state, and local advocacy efforts.
Participate in a Clinical Trial
Volunteering for a clinical trial program can be very valuable. Expensive blood work, treatment medications, and doctor’s visits are usually provided free of charge for those accepted into a study. Clinical trials also provide the opportunity to potentially benefit from the latest advances in medical science.
GlaxoSmithKline is launching a clinical trial, “B-Together,” to study how two drugs (GSK3228836 and Pegasys) might work together to treat chronic hepatitis B (CHB). Researchers hope to find new treatments that could be more effective and lead to positive results that last long after the treatment ends.
You may be eligible to participate in this trial if you are at least 18-years old, have been living with documented CHB for at least six months, and have also been receiving stable nucleos(t)ide treatment (not telbivudine) with no changes for at least six months prior to screening and no planned changes for the duration of the study (79 weeks). This trial is ongoing in the UK, Spain, Russia, Poland, Italy, Korea, Japan, China, the U.S., Canada and South Africa.
Learn more and check your eligibility to participate.
Listen and Learn
Listen to our podcast: B Heppy! This podcast is part of our 300 Million Reasons campaign, a movement to improve awareness about hepatitis B and liver cancer worldwide, to promote engagement of key stakeholders, and to empower people impacted by hepatitis B to become vocal advocates. There are almost 300 million people around the world living with chronic hepatitis B infection, and we want to make sure each and every voice is heard.
Below are the episodes you can listen to, and stay tuned for more episodes about hepatitis B!
COVID-19 and Hepatitis B
The History of the Hepatitis B Foundation and Hep B 101
February 12th marks the start of Lunar New Year and it’s the Year of the Ox! The ox represents hard work, diligence, and honesty.
Sometimes it is so easy to get wrapped up in being diligent at work and neglect your health! If you have not been tested for hepatitis B, you might want to strongly consider knowing your status. If you are living with hepatitis B, be diligent with committing to a healthy lifestyle. Some healthy lifestyle tips include: see your hepatitis B doctor every 6 months to monitor the health of your liver, reduce or eliminate alcohol intake, eat unprocessed foods, avoid smoking or illicit drugs, and exercising.
If you celebrate the Lunar New Year, you might practice some traditions like cleaning your home, setting off firecrackers, watching a lion dance, exchanging red envelopes, and most importantly, a family reunion dinner. Celebrating the New Year might be difficult if you are living with hepatitis B, but you can take steps to celebrate mindfully. Here are some little suggestions for you to consider and possibly incorporate into this year’s celebration:
Making healthier food choices
Try steaming dumplings instead of frying them
Eat more veggie and lean meat dishes
Reduce or eliminate alcohol intake
Not drinking in a social setting can be hard when everyone else is. Some alternatives can include mocktails, non-alcoholic beers, or sparkling water.
In between celebrating, go outside for a little walk around the neighborhood to get some exercise.
Some people living with hepatitis B might be worried about transmitting the virus to their family members through sharing food. The good news is that you cannot transmit hepatitis B through food, water, or even sharing utensils!
If you celebrate the Lunar New Year, we wish you fortune, happiness, and health.
On Monday September 21st, a virtual celebration was held in honor of the sixth anniversary of National African Immigrant and Refugee HIV and Hepatitis Awareness (NAIRHHA) Day. This day, which itself is commemorated on September 9th, was created to build awareness and dismantle stigma around HIV and viral hepatitis in African immigrant and refugee communities. It takes place in September because this is the month that has been designated as National African Immigrant Month (NAIM) in the United States to celebrate the diverse and remarkable contributions African immigrants have made to enrich the United States, in spheres ranging from sports to writing to politics.
The virtual celebration that occurred last Monday included a discussion of the history of NAIRHHA Day and how it came to exist in its present form, a conversation with a hepatitis B advocate who is living with the disease, discourse about the importance of NAIRHHA Day on the national level and implications for making it a federally recognized day, and trivia questions about HIV and hepatitis B.
History of NAIRHHA Day: The Journey from 2014 to Present
Moderator: Chioma Nnaji, MPH, MEd, Program Director, Multicultural AIDS Coalition
Panelists: Augustus Woyah, Program Officer for Minority AIDS Initiative, Maryland Department of Health
Amanda Lugg, Director of Advocacy and LGBTQ Programming, African Services Committee
The idea for NAIRHHA Day was first conceived in 2006 at a convening of the Ethiopian Community Development Corporation in Washington, DC, at a session sponsored by Office of Minority Health about HIV in African immigrant communities. Conferences started to occur, primarily in the Northeast, although there was also interest in Atlanta and Seattle. It seemed that an opportunity had finally become available for advocates, researchers, and providers to all come together and focus on data collection, community mobilization, and policy work around HIV and viral hepatitis in African immigrant communities. The African National HIV/AIDS Alliance was established in 2010 and awareness days started in 2012 (Augustus played a large role in this). In 2014, Chioma Nnaji became connected to Sylvie Bello, the Executive Director of the Cameroonian Association in Washington, DC, and they, along with Amanda and Augustus, worked to get NAIRHHA Day off the ground. Chioma has largely spearheaded efforts to have NAIRHHA Day recognized nationally.
In terms of some of the challenges that have and continue to exist around NAIRHHA Day, obtaining community leadership and organizational buy-in, as well as national attention, are at the forefront. Social media and other digital platforms have been widely used in order to amplify the cause and try to obtain federal recognition. Additionally, maintaining relationships with government agencies has been quite difficult and has become a clash of visions of sorts. There is a strong belief that NAIRHHA Day should be a community-driven effort, but government agencies often have their own priorities, which can be distinct from those of the community and grassroots organizers. This is not to discount the government and organizational partners that are still involved, however, including NASTAD, the Hepatitis B Foundation, CHIPO, CHIPO-NYC, and Africans for Improved Access at the Multicultural AIDS Coalition. Another challenge has been reinforcing the distinction between African immigrant and African American communities and not treating the Black community as a monolith. Drawing this distinction in both data and policy remains difficult, thus often rendering African immigrant communities invisible.
When pondering what areas could use improvement going forward, a number of different items were considered. These included incorporating COVID-19 into the conversation, along with viral hepatitis and HIV; addressing social and environmental determinants of health that lead to the over-prevalence of both infectious and non-communicable diseases in minority, and particularly African immigrant communities; adhering to the primary goal of community mobilization and including advocates and researchers to influence policy that provides linguistically and culturally appropriate services that address the most pressing issue of stigma; securing national attention; and obtaining resources. It is critical to remember that advocacy never ends, the need to magnify work and amplify voices is always present, there is no room for complacency, and there exists intersectionality in all issues (social and health justice are all-encompassing).
#justB Storyteller Interactive Discussion
Moderator: Farma Pene, Community Projects Coordinator in Viral Hepatitis Program, New York City Department of Health & Mental Hygiene
#justB Storyteller: Bright Ansah
In this session, Bright spoke about his experience with living with hepatitis B, including his diagnosis, treatment, and communication with his family. He spoke about being able to put a face to hepatitis B, which has helped many people and also allowed him to build strong relationships with a broader community. Bright found out about his status in 2014 and initially felt very lost. The first couple of years were a big struggle, as he did not want to worry his family and it took a while for him to come to peace with his diagnosis. This peace eventually came from a lot of extensive research, after which he found out that hepatitis B is not a death sentence and can be managed very well. He then started to think about what he could do to prevent someone else from becoming “a statistic.”
When asked what message he would share with newly diagnosed people, Bright stated that stress and anxiety are normal, but you are not alone. Every day, people find out they are infected. Bright has given his contact information to many different people and he emphasized the incredible importance of having a support system in place. When asked about how he overcame stigma and barriers, Bright replied that the biggest barrier is the mental hurdle. It took him about two years to not feel overwhelmed. Bright does still struggle with feeling rejected from clinical trials and finds this very frustrating – he still feels like he is being punished for having chronic hepatitis B.
The best advice that Bright can offer is to always be your own advocate and do your own research. If the first doctor or liver specialist that you find does not take you seriously or you feel that they are not doing enough for you, you do not need to stay with them and you can absolutely find another doctor. Bright went through this process himself and eventually found a doctor he likes at Johns Hopkins, through a friend of his. This can be a challenge with language barriers, but there are organizations that can help and there is a Specialist Directory tool on the Hepatitis B Foundation website, a resource that Bright stated he found very helpful, along with the website of the National Institutes of Health (NIH). Farma reiterated that the HBF website is a great place to visit to understand lab results in plain language, and offers a good collection of resources for family and community members of people living with hepatitis B. Bright finds that the most important questions to ask are: What exactly is your status and viral load? What should reasonable expectations for your life and health be? Is treatment appropriate and if so, which one? It is crucial to establish mutual respect with your doctor, and to iterate what expectations you have for your doctor as well. The most important messages are: Reach out. Ask questions. Stand up for yourself. You are not alone.
The Important Role that NAIRHHA Day Plays from a National and Policy Prospective
Moderator: Chioma Nnaji, MPH, MEd, Program Director, Multicultural AIDS Coalition
Panelists: Boatemaa Ntiri-Reid, JD, MPH, Hepatitis Director, NASTAD
Jennease Hyatt, Community Liaison for Boston/New England, GILEAD
The final conversation focused on why NAIRHHA Day should become a nationally recognized holiday. VIral hepatitis is the seventh leading cause of death globally. Nineteen million African adults are living with hep C, and 5-8% are living with hep B. Hep B and HIV need to be considered part of the health portfolio of African immigrants, with care taken that this does not compound stigma. NAIRHHA Day is really an opportunity to focus on this community specifically. You get things done by doing them yourselves and we are who we’ve been waiting for.
There is a strong need for a multi-faceted approach to this work and for local, state, and national partnerships. African immigrants need to be at the forefront of the HIV/AIDS conversation. In Massachusetts specifically, over half of new HIV infections are in immigrant communities: These communities need to be leading the conversation. In terms of the role that government agencies play in NAIRHHA day, this needs to be more than a supportive role. We need to talk about novel approaches. We know that there are healthcare disparities. We need to consider how to use funding to build capacity and engagement, and make sure this work moves forward. This should include counting in community members and small businesses and bringing people to the table who are not usually there. The community really wants to be engaged. Promoting testing and awareness at soccer games, for example, is a great idea. We need strong partnerships and leadership from the beginning and to determine different approaches and thus different outcomes. Community members are the experts and we need to treat them as such.
Across the country, there are jurisdictions that have a prevalence of 40,000 people living with hepatitis in a state and viral hepatitis staff have teams of 1-7. Local and state health departments have more of a role to play. CDC publishes a list of viral hepatitis coordinators by state. It would be great to close the gap with them and discuss more about what they are doing generally and how to get them more involved in NAIRHHA Day specifically. In thinking about a vision for NAIRHHA Day next year, thoughts included that everyone who serves African immigrant communities (including health centers and multi-service organizations) needs to see themselves as part of the solution. Additionally, federal representation should be part of NAIRHHA Day next year.
Trivia and Conclusion
The event concluded with trivia questions about HIV and hepatitis B prevention, testing, and treatment. Amazing music was provided by DJ WhySham and Laura O (@LauraO_TV) served as an excellent moderator. Thanks to everyone who participated and we look forward to another wonderful event next year!
Infection Control in Dentistry and its Connection to Hepatitis B
Hepatitis B, a major cause of liver damage and liver cancer, is a silent epidemic worldwide. It is a bloodborne infection that is commonly transmitted through blood and sexual fluids. In the dental office, it is mostly transmitted via blood. It is vital to ensure infection control practices are being followed during dental procedures such as cleanings, extractions, injections, root canals, and surgical procedures to reduce the incidence of hepatitis B.
According to a study from the Department of Periodontology and Endodontics at the State University of New York at Buffalo, unvaccinated dental health care workers have a 10 times greater risk of becoming infected with hepatitis B compared to the average citizen because of possible occupational exposure.[1] The CDC recommends that all health care providers, including those working in dentistry, be vaccinated to protect them. Patients can also play a role by ensuring that they are vaccinated as well. The hepatitis B vaccine is safe and effective and protects for a lifetime!
The transmission of hepatitis B in dental surgery can also be prevented by the routine exercise of good clinical hygiene. The dental clinic must properly and routinely dispose of needles, sterilize instruments, and comply with all standard precautions (e.g., wearing appropriate personal protective equipment and disinfecting all equipment and surfaces after each patient) for all patients. In the 2016 update of Transmission of blood-borne pathogens in US dental health care settings, the authors identified lapses in infection prevention practices and failure to adhere to Centers for Disease Control and Prevention (CDC) recommendations as the major causes behind breakouts of hepatitis B in dental settings (see CDC guidelines for the United States here).[2] Examples of lapses included the failure to heat-sterilize handpieces between patients, a lack of training for interns/personnel, and the use of a combination of unsafe injection practices. [2] These reports emphasize the need to improve dental health care personnel’s understanding of the basic principles of infection control.
While at your dentist’s office, you can play a role in ensuring the staff implements proper infection control practices. Before being seated, make sure the chair and all surfaces have been properly wiped down after the previous patient completed treatment. Ensure there is no visible blood or saliva on any surfaces. Before any work is done, ask your dentist if the instruments have been properly disinfected or sterilized. Then, your dentist should take a thorough medical history, asking specific questions about medications, current illnesses, recurrent illnesses, or other infections. Your dentist should also use new protective attire and barrier techniques such as gloves, surgical masks, protective eyewear, and a gown or laboratory coat. In addition, do not be afraid to seek affirmation that the dentist has washed their hands prior to your treatment. When using sharp instruments or needles your dentist should use extraordinary care to prevent unintentional injuries. The needle should be properly disposed of or recapped to decrease the risk of needlestick injury.
The lack of awareness about the importance and dangers of hepatitis B often stems from dental schools. The Himachal Institute of Dental Sciences in Paonta Sahib, India conducted a study which revealed that while dentists are among the high-risk transmission groups for hepatitis, they have little knowledge or information on hepatitis B and/or the vaccine.[3] The study also concluded that proper infection control, sterilization, and prophylactic vaccination protocols should be followed in order to reduce the risk of hepatitis in India.[3] Another study, performed by Saveetha Dental College & Hospital in Chennai, India, evaluated the awareness of the hepatitis B virus among dental graduate students at the University Dental College.[4] A questionnaire regarding the awareness of hepatitis infections and various infection control measures was distributed among all the students in the dental graduate program.4 The data extracted showed that final year students had an increased awareness when compared to third-year students.[4] The overall awareness among the students was unsatisfactory and further signifies the need for continued infection control education.
Similarly, a study performed at Obafemi Awolowo University in Nigeria evaluated the attitude of 120 students towards the hepatitis B vaccine through an anonymous questionnaire.[5] The results showed that of the 94.7% of the students who did not receive the vaccine cited their busy schedule as the reason for their failure to be vaccinated.5 Furthermore, the University of Pretoria in South Africa conducted a study aimed to determine the knowledge among 292 dental students on the transmission and prevention of the hepatitis B virus.[6] It was found that more than 50% of the students did not know that the hepatitis B infection can be transmitted through piercings and more than 50% of the nonclinical students wrongly reported that antibiotics can be used to prevent infection after exposure.6 These studies demonstrate that there is a lack of knowledge surrounding hepatitis B in some dental school settings which contributes to insufficient knowledge about hepatitis B in professional dental settings.
Although awareness about hepatitis B is improving worldwide, dental schools must begin to stress its prominence and importance of infection control in dental settings. It is a good idea for patients to ask about the infection control practices implemented at their dental offices. Emphasis should always be placed on consistent adherence to recommended infection control strategies, and each dental clinic should have a written protocol for instrument reprocessing, operatory cleanup, and management of injuries. Such efforts will lead to the development of safer and more effective medical devices, work practices, and personal protective equipment; all in conjunction decreasing the incidence of hepatitis B.
Guest Author:
Shrey Patel
Bridging the Gaps Intern
Second Year Dental Student at the University of Pennsylvania School of Dental Medicine
References:
[1] Araujo MW, Andreana S. Risk and prevention of transmission of infectious diseases in dentistry. Quintessence Int. 2002;33(5):376-382.
[2] Cleveland JL, Gray SK, Harte JA, Robison VA, Moorman AC, Gooch BF. Transmission of blood-borne pathogens in US dental health care settings: 2016 update. J Am Dent Assoc. 2016;147(9):729-738. doi:10.1016/j.adaj.2016.03.020
[3] Dahiya P, Kamal R, Sharma V, Kaur S. “Hepatitis” – Prevention and management in dental practice. J Educ Health Promot. 2015;4:33. doi: 10.4103/2277-9531.157188. [PubMed: 26097847]. [PubMed Central: PMC4456879].
[4] Mahesh R, Arthi C, Victor S, Ashokkumar S. Hepatitis B infection awareness among dental graduate students: A cross sectional study. Int Sch Res Notices 2014. 2014:1–6.
[5] Adenlewo OJ, Adeosun PO, Fatusi OA. Medical and dental students’ attitude and practice of prevention strategies against hepatitis B virus infection in a Nigerian university. Pan Afr Med J. 2017;28:33. Published 2017 Sep 14. doi:10.11604/pamj.2017.28.33.11662
[6] Madiba T.K., Nkambule N.R., Kungoane T., Bhayat A. Knowledge and Practices Related to Hepatitis B Infection among Dental and Oral Hygiene Students at a University in Pretoria. J. Int. Soc. Prev. Community Dent. 2018;8:200–204. doi: 10.4103/jispcd.JISPCD_31_18.
In the United States, August is National Immunization Awareness Month (NIAM)! During this time, health care providers, educators, and advocates use their resources to inform the public about the safety and importance of vaccines. NIAM was established by the Centers for Disease Control and Prevention (CDC) to encourage individuals of all ages to stay up-to-date with their vaccines and make sure that they are protected. The modern hepatitis B vaccine has been widely used – with over 1 billion doses given – since it was created in 1985, and has been proven to be one of the safest and most effective vaccines in the world. So why do we need to promote the hepatitis B vaccine during NIAM?
United States:
On a national level, vaccination rates for hepatitis B are far below where they should be despite being the most effective way to prevent transmission. In the United States, while 91% of children complete the hepatitis B vaccine series, only 64% of children who are born in hospitals are given the hepatitis B birth dose (first dose of the vaccine) as recommendedby the CDC – which means that there is much room for improvement. And without the follow-up doses, children are still vulnerable to potential exposures; one dose of the vaccine is not enough.
Adults in the United States have extremely low rates of vaccination, primarily because many were born before the vaccine became a healthcare standard and mandated for school. According to the CDC, just 25% of adults have received all three doses. Coupled with the recent increase in injection drug use, low vaccination rates among adults have been driving a rise in acute hepatitis B cases across the nation. The good news is that adults can be fully vaccinated with just 2 doses of the Heplisav-B vaccine! This new vaccine has proven to be highly effective and can be completed in just one month.
Globally:
Internationally, vaccine rates differ from country to country due to issues with storage, access, affordability, general awareness and priorities. In July 2019, the World Health Organization (WHO) announced that 189 countries now provide the vaccine for infants on a national level, but the global coverage of the birth dose is just 42%. The birth dose is significant for a number of reasons. Ninety percent of babies and up to 50% of young children will progress to chronic hepatitis B if they are infected. Since only 10% of the 292 million chronically infected individuals know about their infection, there is the potential for friends or family members to unknowingly transmit the virus to an infant or young child. In addition, a mother who is unaware of her status has the potential to pass the virus to her newborn via the delivery process. The birth dose significantly lowers the risk of transmission in both of the previous scenarios. That is why it is critical pregnant women are tested early in their pregnancy so they are aware of their infection and can ensure the birth dose is available.
In some countries, the pentavalent vaccine is offered. This vaccine protects against five diseases, including hepatitis B. However, it cannot be administered until the baby is at least 6 weeks old, which leaves a gap in the baby’s protection. The monovalent hepatitis B vaccine should be given to all infants in order to make sure they are covered during this vulnerable time period. It is especially important for infants born to hepatitis B surface antigen positive (HBsAg +) mothers to receive the monovalent vaccine within 12-24 hours of birth to prevent transmission.
Vaccines are also essential for healthcare workers. WHO estimates that out of the 3 million healthcare workers who are exposed to bloodborne diseasesa year, approximately 2 million of those exposures are to hepatitis B. These exposures, which largely occur in countries where hepatitis B is common, put unvaccinated healthcare workers at risk. International recommendations list hepatitis B as one of the essential vaccines for health occupations. WHO also reports that unsanitary healthcare practices, such as reusing sharp objects that have not been sterilized following proper infection control practices, were responsible for nearly 2 million hepatitis B infections globally in 2010. Infections from an accidental exposure can easily be avoided with the vaccine!
NIAM is a reminder that a vaccine is only effective at preventing disease when it is used widely. Governments, healthcare providers, and individuals all play an important role in ensuring that people of all ages – especially high-risk individuals – are protected. You can do your part today by asking your doctor for the3-panel hepatitis B blood test. If your results come back negative (HBsAg -, HBsAb -, and HBcAb -), ask them to begin the vaccination series! In two or three simple doses, you can be protected from the largest risk factor for liver disease and liver cancer!
As you may know, two years ago the Hepatitis B Foundation started our Hepatitis B Cure Campaign, to promote increased public-sector investment in hepatitis B and liver cancer research. We have made great progress and wanted to provide an update. Earlier this year, the HBF submitted House Labor-HHS report language, and HBF President Dr. Timothy Block met with the National Institutes of Health’s (NIH) Deputy Director Dr. Lawrence Tabak, to urge the NIH to establish an inter-institute working group to coordinate NIH research focused on finding a cure for hepatitis B and liver cancer.
We are pleased to let you know that due to this outreach, the NIH is establishing a Trans-Institute Hepatitis B Working Group. This Working Group has been tasked with developing a Strategic Plan to Cure Hepatitis B, which Dr. Tabak stated should be a “huge boost” to the shared goal of finding a cure for hepatitis B. The formation of the group follows the NIH’s release in February 2019 of a Request for Information (RFI) that asked members of the research community to provide input on a strategic framework for the Working Group. The RFI suggested the Strategic Plan focus on three areas of research that are essential to developing a cure for hepatitis B:
Understanding Hepatitis B Biology
Developing Tools and Resources
Developing Strategies to Cure Hepatitis B
NIH has reported that there was a very enthusiastic response to the RFI, and they are currently working to finalize an RFI Analysis Report and will include all the responses as an appendix. The report will help to guide the Working Group as they create their strategic elimination plan. Both the Trans-Institute Hepatitis B Cure Strategic Plan and the RFI Analysis Report will be made available to you in the coming months.
This is good news as we work towards finding a cure for hepatitis B. All increased investments help support and implement the goal toeliminate hepatitis B globally.Having new treatments, and especially a cure, will be critical to reach this goal. Seeing the increased interest among the NIH, as well as the nation’s hepatitis B experts and researchers, is an exciting step in the journey to find a cure.
Are you a hepatitis B patient living in the United States? Are you taking entecavir or tenofovir disoproxil fumarate (TDF) to help manage your hepatitis B infection? Thanks to the Hepatitis B Foundation’s new strategic partnership with Rx Outreach – America’s largest fully licensed, non-profit, mail order pharmacy and Patient Assistance Program – you may be able to receive your medication for less than 5% of the average retail price!
Each year, we answer thousands of national and international phone calls, emails, and social media messages from people who have been impacted by hepatitis B. Over the past year, we have seen a significant increase in calls regarding access to medication. The majority of those calls have been from people living in the United States. The ability to access medications is more than just having them available at a local pharmacy – it is about the price as well.
In the United States, life-saving generic treatments can cost more than $830 a month on average. As treatments are typically taken for several years after a person begins, paying such high monthly out-of-pocket costs simply isn’t an option for most people. That’s why we partnered with Rx Outreach to increase patient accessibility to life-saving hepatitis B medications.
We believe that affordable treatments should be low-cost and widely available to everyone who needs them. Hepatitis B antiviral treatments need to be taken daily in order to be effective, and a lack of affordable options force some individuals who are living with chronic hepatitis B to avoid diagnosis and treatment, to stop taking medication or to only take it sporadically, which increases their risk of developing cirrhosis or liver cancer. Our new partnership can help eliminate the need for such potentially harmful actions by providing the same medication at a much lower cost than retail pharmacies, pharmaceutical companies, and insurance plans can offer.
Rx Outreach provides a 30-day supply of entecavir and TDF – two of the most effective, common, and preferred treatments – through the mail. Interested individuals can enroll in the program with 3 simple steps. If you need to transfer your prescription from anotherpharmacy, you can do that too!
Eligibility Requirements:
Eligibility is based upon household income, not on insurance status or prescription drug coverage. To be eligible for Rx Outreach’s pricing, please review the chart below or you can check your eligibility here.If it appears that you do not qualify but you believe that you should, you can also call Rx Outreach and a representative will assist you.
Our partnership with Rx Outreach will help to fill a gap in access to affordable medication and help to lessen the burden of one of the many forms of discrimination that those living with hepatitis B must face. It offers more than 1,000 medication strengths at affordable prices. Since 2010, Rx Outreach has saved people in need more than $662 million on their prescription medication.
North American Occupational Health and Safety Week (May 5-11) is a time to raise awareness about the importance of injury and illness prevention in the workplace! This week, we’re focusing on health and safety within the nail salon industry, specifically the risk for hepatitis B transmission and opportunities to increase awareness and education about hepatitis B among nail salon workers.
In the U.S., the nail salon workforce is comprised mostly of Vietnamese Americans, with many being immigrants. Refugee and immigrant communities are often susceptible to worker exploitation (including labor trafficking) and encounter cultural and linguistic barriers that may leave them vulnerable to occupational health and safety risks, including hepatitis B transmission.
During routine work, nail technicians may be exposed to a client’s blood or other bodily fluids. It is important for nail salon workers to take precautionary measures to protect themselves and their clients to prevent the potential spread of the hepatitis B virus. More importantly, the nail salon industry (including salon owners and state health departments or boards that regulate nail salons) should implement policies that support greater education, awareness, and prevention of hepatitis B transmission among its workforce.
In October of 2011, the American College of Gastroenterology urged the need for increased surveillance and information on disinfection and infectious disease prevention, particularly for hepatitis B and C in nail salons. Since then, no major research or analysis has been conducted to better understand hepatitis B transmission or the policies that protect nail salon workers. In a new report released by the Hepatitis B Foundation, “The Impact of Nail Salon Industry Policies and Regulations on Hepatitis B Awareness and Prevention,” we seek to further understand the nail salon industry landscape through analyzing state policies that govern nail salons and identify strategies to support increased hepatitis B education, awareness, and prevention.
The nail salon industry is regulated at the state level by a regulatory Board of Cosmetology that oversees and ensures nail technicians and nail salons comply with all rules and regulations. In this report, we analyze the nail salon workforce and industry regulations and provide recommendations that can address specific concerns. We conducted phone interviews with health clinics, public health workers, and other relevant stakeholders to better understand the challenges this population encounters when accessing hepatitis B education and care. In addition, we conducted a policy analysis of each state’s Board of Cosmetology to assess their effectiveness in protecting workers from exposure to bloodborne pathogens, specifically hepatitis B. In our analysis, we found that several states may not adequately protect workers from workplace hazards that may increase their risk of hepatitis B exposure. With sanitation and disinfection requirements that greatly vary between states, low compliance can leave workers susceptible to the transmission of bloodborne pathogens, including the hepatitis B virus.
We offered the following recommendations to provide industry changes and community initiatives that can help protect workers or link them to care:
Build partnerships between community organizations and nail salons to increase hepatitis B education, testing, and vaccination among nail salon workers
Integrate hepatitis B education into the nail technician licensing curriculum
Implement continuing education (CE) requirements around hepatitis B prevention and uphold sanitation requirements
Provide multilingual course training materials and written licensing exams
Adopt a sanitation rating system
Additionally, through our analysis, we found that four states have policies that discriminate against nail salon workers affected by hepatitis B by barring them from working in nail salons. Even with federal legal protections from the Americans with Disabilities Act, the continued discrimination in this industry presents a clear need to increase hepatitis B knowledge and awareness. Further state-level advocacy will be needed to address discriminatory policies. We must hold states accountable and advocate for policies and regulations that protect individuals affected by hepatitis B and prevent transmission of hepatitis B in the nail salon workplace.
Be sure to check out our full reportfor a detailed analysis of current state regulations and policies to assess their impact on educating and protecting nail salon workers and preventing hepatitis B transmission in the workplace.
Whether you work in a nail salon or visit one for a manicure or pedicure, be knowledgeable about the steps you can take to protect yourself. For further information about nail salon hazards and a complete guide to protecting your health and preventing injury in the workplace, check out OSHA’s guide here.
Phase 3 clinical trials have been announced for two drugs, Lonafarnib and Myrcludex (Bulevirtide) for the treatment of hepatitis B and delta coinfection.
Phase 3 studies compare new possible treatments to the current standard treatment, to see if it is more effective and/or safer than the current standard of care. Phase 3 studies are randomized control trials, which means that patients will be assigned to one of several different treatment groups. These studies usually evaluate the new treatment over a long period of time but special designations by the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA), such as Fast Track, Orphan Drug, Breakthrough Therapy Designations and PRIME eligibility status will speed up this process and bring these drugs to approval more quickly. Because the only currently approved treatment for hepatitis delta is pegylated interferon, which is often less than 30% effective, there is an unmet need for faster development of more treatment options.
Phase 3 clinical trials for Lonafarnib are currently recruiting hepatitis B and delta coinfected patients in the United States. Ninety-two international trial site locations have also been announced and will take place in Belgium, Bulgaria, Canada, France, Germany, Greece, Israel, Italy, Republic of Moldova, New Zealand, Pakistan, Romania, Span, Switzerland, Taiwan, Turkey, United Kingdom and Vietnam. This clinical trial, run by Eiger Biopharmaceuticals, will test the new drug Lonafarnib in combination with other treatments. For more information about the study, visit www.D-LIVRstudy.comor clinicaltrials.gov.
Bulevirtide, made by MYR-GmbH Pharmaceuticals, has also announced that its phase 3 clinical trials will be opening in 2019. Trial site locations have not been announced yet. For more information about this study, visit clinicaltrials.gov.Click here for more information on locating additional clinical trials. If you are considering joining a clinical trial, discussing it with your liver specialist can be helpful in determining if joining a trial may be right for you.
It is very important for hepatitis B and delta patients to be managed by a doctor, preferably a liver specialist, who is familiar with managing hepatitis B and delta coinfection. For assistance in locating a specialist near you, please visit our Physician Directorypage. For additional questions, please visit www.hepdconnect.org or email connect@hepdconnect.org.




 Infection Control in Dentistry and its Connection to Hepatitis B
Infection Control in Dentistry and its Connection to Hepatitis B safety and importance of vaccines. NIAM was established by the
safety and importance of vaccines. NIAM was established by the 


 The nail salon industry is regulated at the state level by a regulatory Board of Cosmetology that oversees and ensures nail technicians and nail salons comply with all rules and regulations. In this report, we analyze the nail salon workforce and industry regulations and provide recommendations that can address specific concerns. We conducted phone interviews with health clinics, public health workers, and other relevant stakeholders to better understand the challenges this population encounters when accessing hepatitis B education and care. In addition, we conducted a policy analysis of each state’s Board of Cosmetology to assess their effectiveness in protecting workers from exposure to bloodborne pathogens, specifically hepatitis B. In our analysis, we found that several states may not adequately protect workers from workplace hazards that may increase their risk of hepatitis B exposure. With sanitation and disinfection requirements that greatly vary between states, low compliance can leave workers susceptible to the transmission of bloodborne pathogens, including the hepatitis B virus.
The nail salon industry is regulated at the state level by a regulatory Board of Cosmetology that oversees and ensures nail technicians and nail salons comply with all rules and regulations. In this report, we analyze the nail salon workforce and industry regulations and provide recommendations that can address specific concerns. We conducted phone interviews with health clinics, public health workers, and other relevant stakeholders to better understand the challenges this population encounters when accessing hepatitis B education and care. In addition, we conducted a policy analysis of each state’s Board of Cosmetology to assess their effectiveness in protecting workers from exposure to bloodborne pathogens, specifically hepatitis B. In our analysis, we found that several states may not adequately protect workers from workplace hazards that may increase their risk of hepatitis B exposure. With sanitation and disinfection requirements that greatly vary between states, low compliance can leave workers susceptible to the transmission of bloodborne pathogens, including the hepatitis B virus.
 Phase 3 clinical trials have been announced for two drugs,
Phase 3 clinical trials have been announced for two drugs, 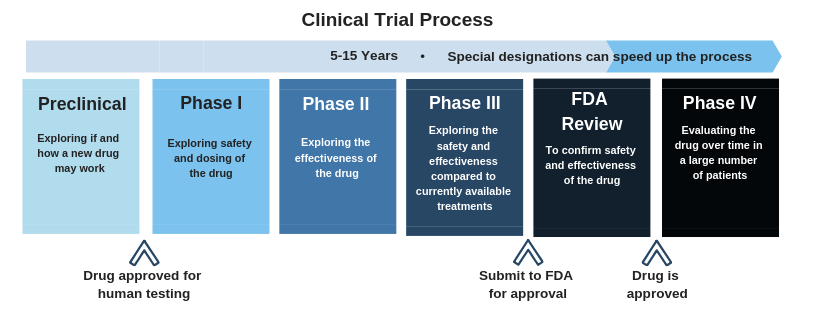 Click here
Click here