
 June is Pride Month in the United States! This month we celebrate the LGBTQ+ community in honor of the 1969 Stonewall Uprising in Manhattan. This blog post will discuss HIV/HBV coinfection in LGBTQ+ individuals and how to prevent both viruses.
June is Pride Month in the United States! This month we celebrate the LGBTQ+ community in honor of the 1969 Stonewall Uprising in Manhattan. This blog post will discuss HIV/HBV coinfection in LGBTQ+ individuals and how to prevent both viruses.
HIV/HBV Co-Infection
Human Immunodeficiency Virus or HIV disproportionately affects LGBTQ+ individuals, mostly gay and bisexual men. In the United States, approximately 69% of the 37,968 new HIV cases were among gay and bisexual men in 2018. HIV can also impact lesbian women, although the infection rate among this community is lower. There is also very limited current data out about lesbian and bisexual women and the burden of HIV. However, HIV can be transmitted between women who have sex with women through sex toys and injection drug use. The CDC reports 1 million people have identified as transgender in the United States, and 2% of those individuals are affected by HIV.
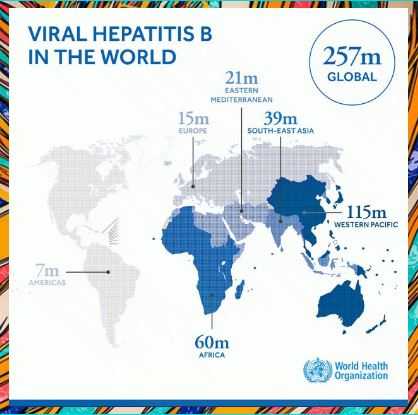
Approximately 5-20% of the HIV-infected population worldwide is also living with hepatitis B. These rates vary among different regions and at-risk populations based on modes of transmission. This figure may approach 20% in Southeast Asia, and 5% in North America and Western Europe. In the U.S., Western Europe, and Australia, the prevalence of chronic hepatitis B was reported to be 5%-14% among HIV-positive individuals.
Since both HIV and the hepatitis B virus share similar transmission routes, it is not surprising that there is a high frequency of coinfection. Sexual activity and/or injection drug use are the most common routes of transmission of the hepatitis B virus among those also infected with HIV.
Prevention
You can easily prevent hepatitis B with a safe and effective vaccine. The vaccine comes in either 2 or 3 doses, given over a span of 6 months. Learn more about the vaccine dose schedule here!
If you are not vaccinated for hepatitis B, ask your doctor or primary care provider for the vaccination! Check out this list of LGBTQ+ friendly providers.
If you are unsure of your hepatitis B status, ask your doctor or primary care provider to become tested! The hepatitis B test is super simple – it only requires one blood sample. Your doctor should order the “hepatitis B panel” which includes different tests. Read more hepatitis B testing here!
You can lower your risk of acquiring HIV by using PrEP (pre-exposure prophylaxis). PrEP is a daily medication you can take to prevent HIV. Just make sure you are tested for hepatitis B before starting PrEP. Read more about PrEP here!
Author: Evangeline Wang
Contact Information: info@hepb.org

 HIV and viral hepatitis. Advocates for NAIRHHA Day recognized the need to address these health issues in the community and thought that a combined awareness day would be the most effective way to reach the largest number of people impacted.
HIV and viral hepatitis. Advocates for NAIRHHA Day recognized the need to address these health issues in the community and thought that a combined awareness day would be the most effective way to reach the largest number of people impacted. 


