Getting poked with a needle is never fun, but it’s an extremely important part of protecting yourself and others from infectious diseases! The hepatitis B vaccine is known to be one of the most effective vaccines in the world – and very safe too! As a blood-borne disease that typically has no symptoms, hepatitis B can easily be spread by accident – simply because people are unaware that they have it! Modes of transmission include mother-to-child during birth, unprotected sex, injection drug use, unsafe medical procedures, and the sharing of personal items that may contain blood remnants, such as body jewelry, razors, and toothbrushes. Although certain precautions can be taken to prevent transmission, the only way to completely protect yourself is to get vaccinated. Once you have been vaccinated, you are protected for life!
There are a few options for receiving the hepatitis B vaccination. In most countries, the vaccine is available through a doctors office or a health clinic. The most common option is the standard three-dose vaccine. This consists of three separate doses of the vaccine given through intramuscular injections. In order for the vaccine to be effective, there must be a minimum amount of time between doses. If the minimum amount of time is not followed, the vaccine will not provide full, long term protection from the infection.
3 Dose Schedule:
- 1st Shot – At any given time, but newborns should receive this dose in the delivery room within 24 hours of birth
- 2nd Shot – At least one month (or 28 days) after the 1st shot
- 3rd Shot – At least 4 months (16 weeks) after the 1st shot (or at least 2 months after the 2nd shot). Infants should be a minimum of 24 weeks old at the time of the 3rd shot.
In the United States, there is an FDA approved 2-dose vaccine called Heplisav-B. However, Heplisav-B is only approved for adults. Both doses must be from the Heplisav-B vaccine only.
2-Dose Schedule (U.S. Only):
- 1st shot – At any given time
- 2nd shot – At least 28 days after the first shot.
Accelerated Vaccine Schedule
At the moment, Heplisav-B is the only vaccine that is approved on a shortened schedule. Some doctors may offer an accelerated vaccine schedule for special circumstances. However, the accelerated schedule is generally not recommended for individuals who do not need the vaccine within a certain time period. The Centers for Disease Control and Prevention only recommends the accelerated vaccine schedule to those who are traveling on short notice and have a high risk of facing exposure, or to emergency responders in disaster areas. Multiple studies have shown that the minimum time between doses is necessary in order to receive full protection against the infection. If doses are given too close together, the body does not have enough time to create an immune response to the vaccine’ leaving you vulnerable to transmission. If you must complete an accelerated schedule, four doses of the vaccine are required in order to achieve full, long-term immunity.
4 Dose Schedule:
-
- 1st Shot – At any given time
- 2nd Shot – 7 days after the first shot
- 3rd Shot – Between 21 and 30 days after the 1st shot
- 4th Shot – 1 year after the first shot
Combined Vaccines
In some cases, the hepatitis B vaccine is administered along with other vaccines or as part of a combination vaccine. Examples of combination vaccines that offer protection against HBV include: 1) The pentavalent vaccine which is used for children and protects against a total of five infectious diseases and 2) the combination hepatitis A and B vaccine. While the pentavalent vaccine is offered as the first dose for children in many countries, it is not ideal unless the child is able to get the birth dose of the HBV vaccine. It can only be given once the child is six weeks old, leaving the infant unprotected during the gap. Therefore, it is strongly recommended that children receive a monovalent hepatitis B dose of the vaccine at birth. For women that are HBsAg positive, the birth dose is the best chance to prevent hepatitis B transmission to the next generation and must be given within 24 hours of birth.
Pentavalent Vaccine Schedule
- 1st Shot – Monovalent at birth
- 2nd Shot- Pentavalent at 2 months of age
- 3rd Shot – Pentavalent at 4 months of age
- 4th Shot – Pentavalent at 6 months of age
The combined hepatitis A & B vaccine – which is only for adults – can follow the 3 dose vaccine schedule or, if necessary, the 4 dose accelerated schedule. More information on combination vaccines can be found here.
Before you get vaccinated, it is important to get tested for hepatitis B! The vaccine will not work for those who are currently infected or have previously been infected. Those who have recovered from a past infection will produce antibodies to the virus and will not have to worry about becoming reinfected or infecting others – but the virus can become reactivated if they undergo immune suppression, so it is important for you and your doctors to know if you have recovered from a past hepatitis B infection. However, those who are currently infected will still be able to transmit the virus – even if they receive the vaccine. Therefore, it is important to know your current status. Ask your doctor or local healthcare provider for the 3-panel hepatitis B blood test (HBsAg,HBsAb,HBcAB) to find out your status today!
 Phase 3 clinical trials have been announced for two drugs,
Phase 3 clinical trials have been announced for two drugs, 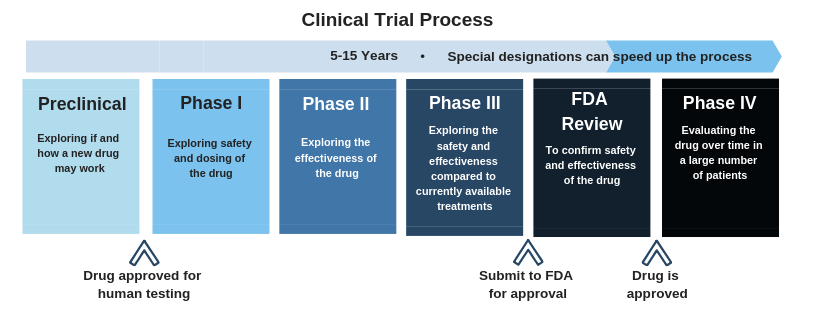 Click here
Click here
 Both issues can impair the liver’s ability to function and filter out toxins that enter the body. They can also increase a person’s risk of developing liver cancer. Recently,
Both issues can impair the liver’s ability to function and filter out toxins that enter the body. They can also increase a person’s risk of developing liver cancer. Recently,